J Educ Community Health. 9(3):176-183.
doi: 10.34172/jech.2022.26
Original Article
The Role of Education in Promoting Safe Motorcycle Riding Behaviors Among Iranian Students: An Application of the Protection Motivation Theory and the Information-Motivation-Behavioral Skills Model
Ali Mehri 1  , Zakieh Sadat Hosseini 2, 3, Abolfazl Davarzani 1, Hadis Barati 1, Hamid Joveini 1, Reza Shahrabadi 1, Masoumeh Hashemian 1, *
, Zakieh Sadat Hosseini 2, 3, Abolfazl Davarzani 1, Hadis Barati 1, Hamid Joveini 1, Reza Shahrabadi 1, Masoumeh Hashemian 1, *
Author information:
1Department of Health Education, Faculty of Health, Sabzevar University of Medical Sciences, Sabzevar, Iran
2Department of Public Health, Neyshabur University of Medical Sciences, Neyshabur, Iran
3Department of Health Education& Health Promotion, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
Abstract
Background: Considering the influential role of teaching safe behaviors in preventing accidents and injuries, this study aims to determine the effect of educational intervention based on protection motivation theory (PMT) and information-motivation-behavioral skills (IMB) model on promoting safe motorcycle riding behaviors in male students at Sabzevar University.
Methods: This quasi-experimental study was performed on 100 motorcyclist students at Sabzevar University selected using two-stage cluster sampling method in 2018. After confirming the validity and reliability of the instrument, the questionnaire was completed three times before, immediately, and two months after the educational intervention. The intervention group was held in 9 educational sessions for three weeks. The data were analyzed by SPSS18 software using t-test, chi-square, Fisher's exact test, and repeated measures tests.
Results: The mean scores of PMT and IMB and safe behaviors of students in the intervention group immediately and two months after the educational intervention compared to the control group showed a statistically significant increase (p<0.001). The mean scores of the studied constructs and safe behaviors in the intervention group had also a statistically significant change over time (p <0.05).
Conclusion: The results indicate the effect of educational intervention based on PMT and IMB on promoting safe behaviors in young students. Face-to-face education and virtual education based on a combination of health education theories can be used to effectively promote safe behaviors of motorcyclist students.
Keywords: Education, Motivation, Motorcycles, Behavior
Copyright and License Information
© 2022 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Mehri A, Hosseini ZS, Davarzani A, Barati H, Joveini H, Shahrabadi R, et al. The role of education in promoting safe motorcycle riding behaviors among iranian students: an application of the protection motivation theory and the informationmotivation-behavioral skills model. J Educ Community Health. 2022; 9(3):176-183. doi:10.34172/jech.2022.26
Introduction
Car accidents are one of the leading causes of death worldwide. According to the World Health Organization, between 20 and 50 million people are disabled as a result of traffic accidents (1). Accidents are currently the eighth leading cause of death in the world, and the 15-29 age group is the most affected group by motorcycle accidents (2). A car accident is the third leading cause of death in Iran after cardiovascular disease and stroke. Three to four hundred thousand people die as a result of motorcycle accidents (3). Motorcycle accidents account for 42% of accidents in Iran (4), and traffic accidents are the second leading cause of death in Sabzevar (5).
The motorcycle is a type of motor vehicle that is of great importance due to its low price, low fuel consumption, high maneuverability, and less road space (6). In high-income countries, the death toll from motorcycle accidents is 5%-18%. However, in low- and middle-income countries, the death rate caused by high motorcycle ownership and accidents is high (7). The highest proportion of victims of motorcycle accidents belongs to urban and rural areas (8,9).
High-risk behaviors such as mental imbalance, lack of adequate training and skills, disregard for traffic rules, alcohol and drug use, and failure to use safety systems, including seat belts and helmets, are the most important human factors in the occurrence of accidents (10). Men as a productive force of society have a key role in the national economy and per capita income, which can help the economy of the family and society in addition to psychological and physical effects on the injured (11). Zare et al emphasized the effective role of education in the use of safety equipment such as helmets, clothing, gloves, and shoes for motorcyclists (12). The use of safety equipment and helmets reduces the risk of death (13). In this regard, one of the best ways to reduce unsafe behaviors is through educational interventions. The effectiveness of educational interventions and health education programs requires the correct and appropriate use of theories and models of health education (14). Many studies have pointed to the effective role of the protection motivation theory (PMT) and information-motivation-behavioral skills (IMB) model in the use of safe and healthy behaviors (15,16). In the PMT, threat appraisal depends on several factors, including the severely problematic (perceived severity) nature of one’s belief, estimation of the individual’s risk of developing the disease (perceived vulnerability), and one’s belief in the positive aspects of unhealthy behaviors (perceived reward). Thus, if perceived severity and vulnerability are high and the perceived reward is low, there will be a stronger motivation to engage in health-promoting behaviors. In the PMT, coping appraisal involves evaluating the effectiveness of protective behavior in dealing with a threat (response effectiveness), including belief in one’s ability to manage protective behaviors (self-efficacy), the individual’s estimation of costs (including money, time, and energy), and efforts to perform protective behaviors (response costs). It is expected to enhance the effectiveness of the response and the self-efficacy of the coping appraisal, while it is expected to reduce the response cost. Fear mediates between perceived vulnerability, perceived severity, and threat appraisal. Accepting the recommended safe behavior is assumed to be a direct act of motivation to protect oneself. To be called protective motivation, perceived severity, vulnerability, self-efficacy, and response efficiency must overcome fixed costs and rewards (17). The IMB model assumes that the implementation of a health promotion behavior is a function of the individual’s full awareness of the behavior, the motivation to engage in the behavior (e.g., having a positive behavior), personal intentional attitude toward behavior, and social support of behavior, and has appropriate behavioral skills to perform the behavior (18). Due to the lack of theory-based educational interventions among motorcyclists in Sabzevar, this study sought to determine the effect of face-to-face and virtual educational interventions on preventing students’ unsafe motorcycle riding behaviors based on a combination of these two models in Sabzevar in 2018.
Materials and Methods
The present quasi-experimental study was conducted among male students of Sabzevar universities (Islamic Azad University, Imam Khomeini Technical University, Hakim Sabzevari University, University of Medical Sciences, the University of New Technologies, and Comprehensive University of Applied Sciences) in 2018, and the research community included all male students of Sabzevar universities. The estimated sample size was based on the study by Mahmoud Abad et al (19) and the following formula.
µ1 = 95.26, µ2 = 88.81, 5.48 =
, 13.47 =
, power = 0.8, and α = 0.05
Taking into account 25% of falls, the sample size in each group was estimated to be 50 people. The samples were selected using a two-stage cluster sampling method so that two universities were randomly selected from the six universities in Sabzevar. Then, 50 subjects were randomly selected from each university. The researcher identified the subjects among those who parked their motorcycles in the parking lot of universities, and they were asked to introduce other motorcyclist students. A list of all motorcyclist students was prepared, and their contact numbers were obtained as well. Overall, 100 students, who had consent to participate in the study, were selected from 2 selected universities and were included in the intervention (n = 50) and control (n = 50) groups after completing the questionnaire. After receiving the code of ethics, the researcher explained to the participants how to perform the plan, the confidentiality of information, and the purpose. The students entered the study after giving informed consent (Figure 1). The inclusion criteria consisted of being in the age range of 18-35 years, having a motorcycle, being a student of the target university, having at least one semester to the end of the study, having a mobile phone, having the ability to use cyberspace to read written texts, and having at least one year of motorcycle driving experience. On the other hand, the exclusion criteria included expressing dissatisfaction to continue cooperation, absence of more than two sessions in educational sessions, and incomplete questionnaires.
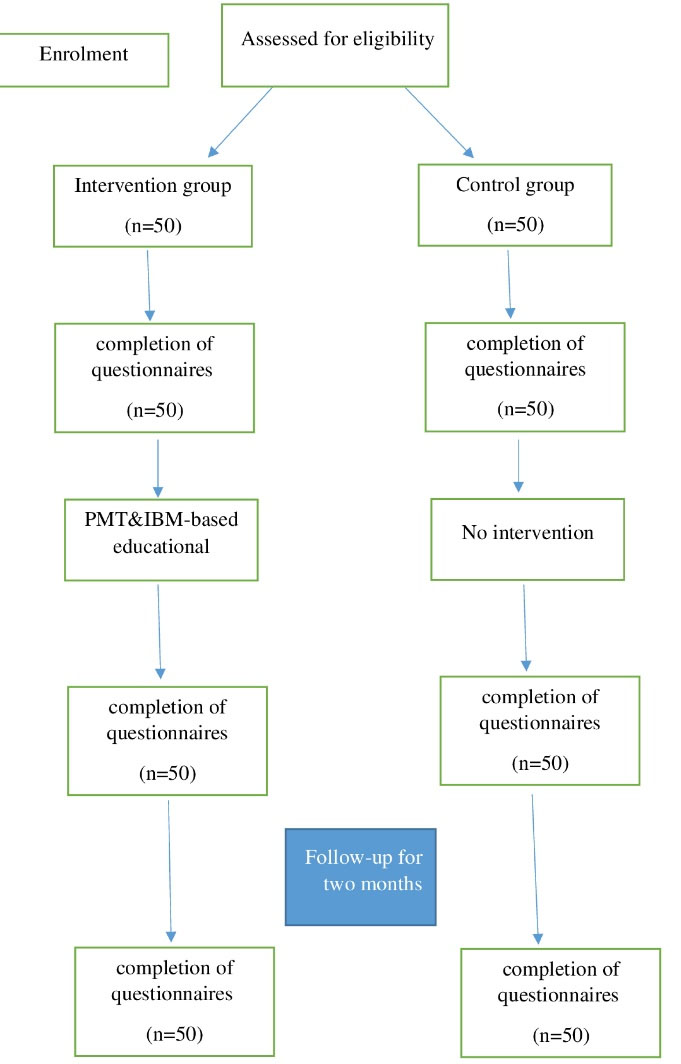
Figure 1.
Steps of Implementing the Research Plan. Note. PMT: Protection motivation theory; IBM: Information-motivation-behavioral skills
.
Steps of Implementing the Research Plan. Note. PMT: Protection motivation theory; IBM: Information-motivation-behavioral skills
The questionnaire had three parts. The first part was related to demographic characteristics, including marital status, the number of family members, monthly family income (Toman), age, place of residence, having a certificate, and parents’ education level. This part also included questions such as “Do you have a history of being fined for riding a motorcycle?” “Do you have a motorcycle license?”. The second part of the questionnaire contained the subscales of the PMT and IMB model. The perceived vulnerability had 7 questions such as “There is a possibility of a motorcyclist crashing at any moment while driving a motorcycle” with a range of 7-35. Perceived severity had 6 questions such as “There is a possibility of death following a motorcycle accident” and self-efficacy had 6 questions such as “I can use a helmet to prevent the complications of a motorcycle accident”. Perceived cost included 6 questions such as “Visually restrictive helmet” and motivation had 6 questions such as “From now on, I intend to use a suitable and standard helmet” with a score range of 6-30. Response efficiency and fear each had 4 questions, including “Wearing a helmet reduces the risk of brain injury for the rider” and “I’m afraid of being fined”, respectively, with a score range of 4-20. Perceived reward contained 5 questions such as “I enjoy riding a motorcycle at high speed” with a score range of 5-25. The subscales of the IMB model had 7 questions such as “I know the allowable speed in different parts of the city” with a score range of 7-35, and behavioral skills included 6 questions such as “I check my motorcycle periodically once a month” with a score range of 6-30. Further, motivation had 5 questions such as “I feel safer by following the traffic rules” with a score range of 5-25. The answers of the studied constructs were categorized based on a 5-point Likert-type scale from strongly disagree (1 point) to strongly agree (5 points). The third part of the questionnaire had 5 questions related to the domain of safe behaviors, and the answers always ranged from 5 to 1 (never).
To have face validity, a face-to-face interview was conducted with ten 18-35-year old motorcyclist students. For example, in the case of a perceived severity construct, the question was “What are the consequences of a motorcycle accident for you?”, and the most critical factors were identified after analysis. In this study, the validity of the questionnaire was based on the opinions of 11 experts in health education and health promotion. The content index score of the present study was calculated as 0.70-0.79. It was found that the effect of overt and covert variables was also significant in the majority of constructs (P < 0.05). The Cronbach’s alpha coefficient was obtained for perceived vulnerability (0.76), perceived severity (0.85), perceived reward (0.76), fear (0.71), self-efficacy (0.9), response efficiency (0.87), perceived cost (0.79), information (0.87), motivation (0.94), and behavioral skills (0.70). To determine the internal stability coefficient of the questionnaires among 30 selected motorcyclist students, who were not in the final study, the range of stability coefficient values obtained in the present study was between 0.78 and 0.91.
The educational content for the intervention group was adjusted after determining the most important predictors of preventive behaviors through multiple regression tests. They included the constructs of perceived vulnerability, perceived severity, self-efficacy, fear, information, behavioral skills, and motivation. Then, the target group was randomly divided into control and intervention groups. In the intervention group, two sessions were held every week for nine sessions of 1.5 hours with the presence of a health education and health promotion specialist. A meeting was held at the university meeting hall, and various educational methods were used according to the target constructs, including group discussion, brainstorming, lectures, questions, and answers, which consisted of educational materials such as film screenings. Educational posters and booklets (Table 1) were employed as well (17). Moreover, the intervention group was divided into two groups of 25 people to participate in educational sessions.
Table 1.
Educational Program in the Intervention Group
|
Sessions
|
Objectives
|
A Summary of Topics and Activities
|
Education Time
|
| First |
Increasing perceived vulnerability |
- Providing explanations about the rules and regulations of the training sessions, the purpose of the study, and the duties of the participants
- Reporting statistics related to the incidence of accidents in motorcyclists
- Discussing young people’s misconceptions about not being vulnerable to unsafe behaviors |
90 |
| Second |
Increasing perceived severity |
- Explaining the lasting problems caused by accidents on motorcycle riders
- Playing clips of the side effects and consequences of not observing safe behaviors in young people |
90 |
| Third |
Reducing perceived rewards |
- Using the brainstorming method to express the perceived rewards of not using safe behaviors and providing the necessary solutions |
90 |
| Fourth |
Increasing fear and
response efficacy |
- Stating bitter experiences caused by a motorcycle accident by a student invited to the meeting
- Brainstorming on how to use safe behaviors while riding a motorcycle
- Providing pamphlets on all safe behaviors on motorcycles |
90 |
| Fifth |
Reducing perceived costs |
-Discussing barriers to using safe behaviors and how to overcome them
- Discussing the positive and negative feelings of participants in the use of safe behaviors |
90 |
| Sixth |
Increasing motivation and self-efficacy |
- Displaying educational clips to teach step by step how to use safe behaviors for students |
90 |
| Seventh |
Increasing information |
- Explaining necessary information about the driving rules and safe speed of the motorcycle
- Providing pamphlets and educational tracts on traffic rules for motorcyclists |
90 |
| Eighth |
Increasing behavioral skills |
Discussing the required skills to assess the safety status of the motorcycle |
90 |
| Ninth |
- Summarizing and reviewing the material mentioned in the previous sessions on how to use safe behaviors while riding a motorcycle. |
90 |
Post-test was performed by redistributing the questionnaire immediately and two months after the educational intervention for both control and intervention groups.
Mean (standard deviation, SD) was used to describe quantitative variables according to conditions, and frequency report (percentage) was applied for qualitative variables. Data were analyzed using an independent t test, chi-square, Fisher’s exact test, and repeated measures analysis of variance (ANOVA). The significance level was considered less than 0.05.
Results
The mean (SD) age of study participants was 19.17 ( ± 2.34) years. Most students (90%) were single, 47.8% of motorcyclist students had never worn a helmet while riding a motorcycle, and 30.4% of them had no driver’s license. Moreover, 57.6% of the subjects used a mobile phone while riding a motorcycle, and more than 21% always went through a red light. The most common reason for students being fined by the police was not wearing a helmet (33%) and unauthorized speed (21%). Approximately 77% of motorcyclist students had a driver’s license. The duration of motorcycle use in 44% of the target population was three years. There was no statistically significant difference between the two groups regarding demographic variables before the educational intervention (P > 0.05, Table 2).
Table 2.
Demographic Variables Between the Two Groups Before the Educational Intervention
|
Variable
|
Group
|
Control Group (n=50)
|
Intervention Group (n=50)
|
P
Value
|
|
Number
|
Percent
|
Number
|
Percent
|
| Marital status |
Single |
43 |
91.48 |
40 |
88.88 |
0.675 |
| Married |
7 |
8.52 |
10 |
11.12 |
| Number of family members |
Two |
0 |
0 |
8 |
66.6 |
0.358 |
| Three |
2 |
4.25 |
17 |
37.77 |
| Four |
22 |
42.22 |
10 |
22.22 |
| Five and more |
26 |
57.77 |
15 |
33.33 |
| No |
26 |
28.30 |
23 |
9.80 |
| Monthly family income (Toman) |
< 0.5 million |
6 |
8.51 |
1 |
2.22 |
0.122 |
| 0.5-1 million |
5 |
10.63 |
14 |
22.22 |
| > 1 million |
39 |
80.85 |
35 |
82.22 |
| Age (y) |
18-20 |
24 |
44.86 |
33 |
73.33 |
0.132 |
| 21-23 |
13 |
27.65 |
8 |
6.66 |
| ≥ 24 |
13 |
27.65 |
9 |
20 |
| Location |
Suburbs |
8 |
63.10 |
11 |
33.13 |
0.469 |
| City |
42 |
36.89 |
39 |
66.86 |
| Having a certificate |
Yes |
35 |
43.37 |
36 |
43.37 |
0.893 |
| No |
15 |
56.63 |
14 |
56.63 |
| Father’s education |
Illiterate |
0 |
0 |
8 |
7.60 |
0.217 |
| Elementary and middle school |
19 |
18.50 |
22 |
21.70 |
| High school and diploma |
26 |
27.20 |
17 |
16.30 |
| Above diploma and university |
5 |
5.40 |
3 |
3.30 |
| Mother’s education |
Illiterate |
3 |
6.38 |
7 |
8.88 |
0.316 |
| Elementary and middle school |
24 |
44.68 |
25 |
55.55 |
| High school and diploma |
14 |
29.78 |
12 |
20 |
| Above diploma and university |
9 |
19.14 |
6 |
11.11 |
Although the mean scores of the constructs before the educational intervention were not statistically significant between the two groups, the independent t test showed that the mean scores of the constructs and safe behaviors immediately and between the two groups had a statistically significant difference two months after the educational intervention (P < 0.05). The results of the repeated measures ANOVA demonstrated that the mean scores of the constructs and safe behaviors in the intervention group had a statistically significant change over time (P < 0.05, Table 3).
Table 3.
Comparison of the Effectiveness of Intervention Program Based on the PMT and IMB Before, Immediately, and Two Months After the Intervention Between the Two Groups
|
Variables
|
Before Intervention
|
After Intervention
|
Two Months After Intervention
|
P
value**
|
|
Mean±SD
|
Mean±SD
|
Mean±SD
|
| Perceivedvulnerability |
Control |
25.25 ± 3.34 |
25.19 ± 3.66 |
24.95 ± 3.50 |
0.325 |
| Intervention |
25.51 ± 2.67 |
33.24 ± 1.29 |
33.71 ± 1.19 |
< 0.001 |
|
P value* |
0.338 |
< 0.001 |
0.004 |
|
| Perceivedseverity |
Control |
22.42 ± 3.61 |
22.34 ± 3.54 |
22.34 ± 2.54 |
0.341 |
| Intervention |
24.64 ± 3.17 |
27.76 ± 1.50 |
28.51 ± 1.50 |
< 0.001 |
|
P value* |
0.356 |
< 0.001 |
0.002 |
|
| Self-efficacy |
Control |
22.95 ± 2.48 |
22.78 ± 2.61 |
22.78 ± 2.51 |
0.221 |
| Intervention |
23.97 ± 4.57 |
27.68 ± 1.68 |
28.06 ± 1.61 |
< 0.001 |
|
P value* |
0.139 |
< 0.001 |
< 0.001 |
|
| Response efficiency |
Control |
15.78 ± 2.04 |
15.61 ± 2.25 |
15.66 ± 2.65 |
0.237 |
| Intervention |
17.36 ± 2.67 |
18.82 ± 1.09 |
19.00 ± 1.02 |
< 0.001 |
|
P value* |
0.256 |
0.002 |
0.003 |
|
| Cost |
Control |
20.95 ± 4.41 |
20.36 ± 5.15 |
20.51 ± 4.33 |
0.265 |
| Intervention |
23.37 ± 1.04 |
28.44 ± 1.28 |
28.95 ± 0.97 |
< 0.001 |
|
P value* |
0.230 |
< 0.001 |
0.004 |
|
| Motivation |
Control |
40.44 ± 4.43 |
40.97 ± 7.04 |
40.42 ± 7.61 |
0.233 |
| Intervention |
40.52 ± 10.70 |
52.43 ± 1.18 |
52.80 ± 1.53 |
< 0.001 |
|
P value* |
0.278 |
< 0.001 |
0.003 |
|
| Perceived Reward |
Control |
16.48 ± 5.66 |
16.91 ± 5.11 |
16.92 ± 5.15 |
0.212 |
| Intervention |
22.17 ± 1.61 |
22.95 ± 1.51 |
23.60 ± 1.06 |
< 0.001 |
|
P value* |
0.254 |
< 0.001 |
0.002 |
|
| Fear |
Control |
15.10 ± 1.43 |
15.59 ± 3.44 |
15.61 ± 3.42 |
0.337 |
| Intervention |
15.62 ± 4.53 |
19.04 ± 3.71 |
19.42 ± 3.61 |
< 0.001 |
|
P value* |
0.359 |
< 0.001 |
< 0.001 |
|
| Information |
Control |
15.57 ± 5.31 |
17.50 ± 5.48 |
17.50 ± 5.61 |
0.326 |
| Intervention |
17.62 ± 4.31 |
24.42 ± 2.61 |
24.22 ± 3.51 |
< 0.001 |
|
P value* |
0.339 |
< 0.001 |
0.004 |
|
| Behavioral skills |
Control |
21.64 ± 3.29 |
21.62 ± 3.19 |
21.80 ± 3.31 |
0.127 |
| Intervention |
23.02 ± 3.61 |
29.24 ± 1.20 |
26.42 ± 1.61 |
< 0.001 |
|
P value* |
0.232 |
< 0.001 |
0.002 |
|
| Behavior |
Control |
23.76 ± 4.93 |
23.72 ± 4.81 |
24.10 ± 4.65 |
0.353 |
| Intervention |
20.24 ± 4.58 |
27.31 ± 4.91 |
34.17 ± 3.01 |
< 0.001 |
|
P value* |
0.338 |
< 0.001 |
0.004 |
|
Note. PMT: Protection motivation theory; IBM: Information-motivation-behavioral skills.
*
P values obtained by comparing differences in the variable values between the two groups using independent t-test; **P values obtained by comparing means in the variable values within each group using repeated measures analysis of variance.
Discussion
According to the findings, nearly half of the participants had never worn a helmet at all, and the lack of a helmet and speeding was the main reason for students being fined. In another study, it was reported that nearly 64% of motorcyclists did not observe the speed limit while driving. The results of studies by Mokhtari et al and Oruogi et al (20,21) on motorcyclists are in line with those of the present study. However, Li et al found that more than 90% of motorcyclists wear helmets. The reasons for the inconsistency with the present study are differences in the geographical area, sample size, and survey method (22). It seems that performing theory-based educational interventions in a codified way is highly effective. By acquiring the necessary skills, performing safe behaviors while driving becomes a part of students’ lifestyles and traffic culture.
According to the findings, immediately and two months after the educational intervention, there was a statistically significant difference in the mean score of threat appraisal between the two groups. The findings of some studies (23-25) are in conformity with the results of the present study, while Rafiei et al reported no significant difference in the perceived severity construct between the two groups after the educational intervention. Such inconsistencies in the results of some studies with those of the present study are differences in the sample size and mean age of the participants and differences in the number of the held sessions (26). During the educational sessions, the study was conducted by providing statistics and information related to the rate of accidents due to unsafe behaviors in young people and the wide consequences of these behaviors during their lives, as well as inviting people who suffer from injuries caused by using unsafe behaviors. The students also expressed the most important rewards they received for performing unsafe behaviors, and then necessary solutions were provided to them through a group discussion.
The results of this study revealed a significant increase in the mean score of coping appraisal immediately and two months after the educational intervention in the intervention group. The mean scores of perceived response efficiency and perceived self-efficacy increased after the educational intervention. However, the costs of performing safe behaviors while riding a motorcycle in the intervention group decreased significantly compared to the control group. The results of some studies by Mirkarimi et al, Baghiani Moghaddam et al, and Bai et al (27-29) are consistent with this finding. Conversely, Dehdari et al did not report a statistically significant change in the mean scores of perceived response efficiency and perceived cost between the two groups after the educational intervention. It can be attributed to the difference during the educational intervention, the type of research, and the study population (30). Participants in the study of Orouji et al stated that the most critical barriers to not wearing a helmet while riding a motorcycle are sweating, hearing impairment, high cost, heaviness, and visual impairment (31). In the present study, using the method of brainstorming, the participants attempted to name their most essential obstacles in using safe behaviors while riding a motorcycle. In return, practical solutions to overcome these obstacles were presented to them. The advantages of safe behaviors in preventing traffic accidents were discussed during the educational sessions.
The present study results showed a significant increase in the mean scores of the information and behavioral skills of students immediately and two months after the educational intervention in the intervention group. In the study by Foster (32), the educational intervention mean scores of information and skills of AIDS-preventing behaviors in truck drivers increased significantly. Anderson et al also found that the level of motivation and behavioral skills increased after educational interventions (16). It was due to the fact that before the educational intervention, students did not know enough about the consequences of unsafe behaviors while riding a motorcycle (e.g., high speed, dramatic movements, lack of helmets, and the like). During the educational sessions, various educational methods, posters, educational pamphlets, and clips were used to increase their information, and each of the skills required to apply safe behaviors was addressed as well.
According to the findings, the mean score of motivation and self-efficacy of students immediately and two months after the educational intervention in the intervention group was significantly higher than in the control group. Numerous domestic and foreign studies confirmed the effect of educational intervention on improving motivation and self-efficacy (33-36). Soltani et al emphasized the influential role of self-confidence and self-efficacy in using safe behaviors in front seat passengers (37). A high sense of self-efficacy will lead to more effort and flexibility to perform safe behaviors more effectively while riding a motorcycle.
According to the results, only 5% of the participants always wore helmets before the educational intervention, and other safe behaviors of the students in the present study did not have the desired level before the educational intervention. This result is in line with the finding of a study by Shahbazzadeh et al, in which 12.6% of Ardabil motorcyclists used helmets (38). In the present study, immediately and two months after the educational intervention, the mean scores of safe behaviors of students in the intervention group were significant compared to the control group. It makes sense when students receive structured educational programs to increase the right information and raise their awareness of safe behaviors and ways to overcome barriers to safe behaviors and their ability. Knowing how to overcome obstacles, believing in them, and using behavioral skills and tools can lead to safe behaviors (39-41).
One of the limitations of the present study is the completion of a self-report questionnaire. Another limitation was the interference of students’ classroom programs with the program of educational intervention sessions, which the researcher tried to overcome through written planning. The simultaneous use of two structured theories during educational sessions and the use of face-to-face education, along with virtual education are among the advantages of this study.
Conclusion
Based on the study results, educational programs based on PMT and IMB could effectively promote safe behaviors in young students. The use of face-to-face education and virtual education combined with the theory of health education and the application of various educational methods will effectively promote the safe behaviors of motorcyclists.
Acknowledgments
Thanks are owed to all students who participated in this study.
Authors’ Contribution
Methodology: MA; Investigation and Validation: AD; Writing-Original Draft Preparation: ZSH; Formal Analysis: HB; Writing-Review and Editing: HJ; Data Curation: RS; Supervision: MH.
Conflict of Interests
The authors declare that there is no conflict of interest.
Ethical Permissions
The Research Ethics Committee of Sabzevar University of Medical Sciences approved this study with the ID: IR.MEDSAB.REC.1397.057.
Funding/Support
This article is retrieved from the research project approved by Sabzevar University of Medical Sciences with project number 97092, which was supported by Vice-Chancellor for Research and Technology of this university.
References
- Sánchez González MP, Escribano Sotos F, Tejada Ponce Á. Impact of provincial characteristics on the number of traffic accident victims on interurban roads in Spain. Accid Anal Prev 2018; 118:178-89. doi: 10.1016/j.aap.2018.02.015 [Crossref] [ Google Scholar]
- Sayyed Hoseinian SH, Ebrahimzadeh MH, Peivandi MT, Bagheri F, Hasani J, Golshan S. Injury patterns among motorcyclist trauma patients: a cross sectional study on 4200 patients. Arch Bone Jt Surg 2019; 7(4):367-72. [ Google Scholar]
- Moghisi A, Mohammadi R, Svanstrom L. Motorcyclists’ safety in Iran: implication of haddon matrix in safe community setting. Med J Islam Repub Iran 2014; 28:37. [ Google Scholar]
- Heydari ST, Bagheri Lankarani K, Vossoughi M, Javanmardi K, Sarikhani Y, Mahjoor K. The prevalence and effective factors of crash helmet usage among motorcyclists in Iran. J Inj Violence Res 2016; 8(1):1-5. doi: 10.5249/jivr.v8i1.667 [Crossref] [ Google Scholar]
- Ghorbani A, Nabavi Fard H, Khoshhal M, Husseini SH. Imposed costs due to traffic accident fatalities (a case study of Sabzevar). Traffic Management Studies 2011;5(20): 49-58. [Persian].
- Zamani Alavijeh F, Niknami S, Mohammadi I, Montazeri A, Ahmadi F, Ghofranipour F, et al. High risk behaviors among Iranian motorcyclists: a qualitative study. Payesh 2010;9(3):269-78. [Persian].
- Ghorashi Z, Kazemi M, Sayyadi AR, Nikbakht Nasrabadi A. Experience of motorcycle accident victims: a qualitative study. J Rafsanjan Univ Med Sci 2012;11(2):115-27. [Persian].
- Gholamaliee B, Khazaei S, Jamorpour S, Mohammadian Hafshejani A, Salehinia H. Epidemiological assessing of motorcyclists’ country-level traffic accidents, 2013. Pajouhan Sci J 2015;14(1):12-21. [Persian].
- Delamou A, Kourouma K, Camara BS, Kolie D, Grovogui FM, El Ayadi AM. Motorcycle accidents and their outcomes amongst victims admitted to health facilities in Guinea: a cross-sectional study. Adv Prev Med 2020; 2020:1506148. doi: 10.1155/2020/1506148 [Crossref] [ Google Scholar]
- Spoerri A, Egger M, von Elm E. Mortality from road traffic accidents in Switzerland: longitudinal and spatial analyses. Accid Anal Prev 2011; 43(1):40-8. doi: 10.1016/j.aap.2010.06.009 [Crossref] [ Google Scholar]
- Davarzani A, Mehri A, Barati H, Joveyni H, Shahrabadi R, Hashemian M. Design and psychometric of measurement tool of unsafe behaviors in motorcycle driving based on information, motivation and behavioral skills model. J Educ Community Health 2019; 6(4):231-7. doi: 10.29252/jech.6.4.231.[Persian] [Crossref] [ Google Scholar]
- Zare H, Mohammadzadeh Edmollaii R, Alipuor A, Tarkhan M. Effectiveness of training in safety riding program on motorcycle rider use of safety equipment. Journal of Safety Promotion and Injury Prevention 2015;3(2):117-26. [Persian].
- Fan HP, Chiu WT, Lin MR. Effects of helmet nonuse and seating position on patterns and severity of injuries in child motorcycle passengers. BMC Public Health 2019; 19(1):1070. doi: 10.1186/s12889-019-7434-5 [Crossref] [ Google Scholar]
- Tazval J, Ghafari M, Mohtashami Yeganeh F, Babazadeh T, Rabati R. Efficiency of protection motivation theory on prediction of skin cancer and sunlight preventive behaviors in farmers in Ilam county. J Health 2016;7(5):656-7. [Persian].
- Sharma HL, Nasa G. Academic self-efficacy: a reliable predictor of educational performances. Br J Educ 2014; 2(3):57-64. [ Google Scholar]
- Anderson ES, Wagstaff DA, Heckman TG. Information-Motivation-Behavioral Skills (IMB) Model: testing direct and mediated treatment effects on condom use among women in low-income housing. Ann Behav Med 2006; 31(1):70-79. doi: 10.1207/s15324796abm3101_11 [Crossref] [ Google Scholar]
- Saffari M, Shojaeizadeh D, Ghofranipour F, Heydarnia A, Pakpour A. Health Education & Promotion-Theories, Models & Methods. Tehran: Sobhan Pub; 2012. p. 234. [Persian].
- Bian C, Xu S, Wang H, Li N, Wu J, Zhao Y. A study on the application of the information-motivation-behavioral skills (IMB) model on rational drug use behavior among second-level hospital outpatients in Anhui, China. PLoS One 2015; 10(8):e0135782. doi: 10.1371/journal.pone.0135782 [Crossref] [ Google Scholar]
- Mazloomimahmoodabad SS, Mehri Morovati MA, Fallah H. Implementation of planned behavior model developed to predict the use of helmets on motorcyclists employees Yazd. J Birjand Univ Med Sci 2007;14(4):356-81. [Persian].
- Orouji MA, Charkazi A, Hazavehei SMM, Moazeni M. Practice of motorcycle drivers on helmet use based on health belief model in khomein city, 2010 2012;3(2):24-31.
- Mokhtari AM, Samadi S, Hatami SE, Jalilian H, Khanjani N. Investigating the rate of helmet use and the related factors among motorcyclists in Kerman between 1391-92 (2012). Journal of Safety Promotion and Injury Prevention 2014;2(3):209-14. [Persian].
- Li Q, Adetunji O, Pham CV, Tran NT, Chan E, Bachani AM. Helmet use among motorcycle riders in Ho Chi Minh City, Vietnam: results of a five-year repeated cross-sectional study. Accid Anal Prev 2020; 144:105642. doi: 10.1016/j.aap.2020.105642 [Crossref] [ Google Scholar]
- Ezzati E, Shariat F, Moradi F, Babazadeh T. The effect of a blended educational program (BEP) on cervical cancer screening behavior among housekeeper women in West Eslamabad in 2016: an application of health belief model. J Ilam Univ Med Sci 2017; 25(1):110-20. doi: 10.29252/sjimu.25.1.110.[Persian] [Crossref] [ Google Scholar]
- Wang Y, Liang J, Yang J, Ma X, Li X, Wu J. Analysis of the environmental behavior of farmers for non-point source pollution control and management: an integration of the theory of planned behavior and the protection motivation theory. J Environ Manage 2019; 237:15-23. doi: 10.1016/j.jenvman.2019.02.070 [Crossref] [ Google Scholar]
- Ghahremani L, Khiyali Harami Z, Kaveh MH, Keshavarzi S. Investigation of the role of training health volunteers in promoting pap smear test use among Iranian women based on the protection motivation theory. Asian Pac J Cancer Prev 2016; 17(3):1157-62. [ Google Scholar]
- Rafiei N, Aghapoor S, Behnampour N, Heshmati H, Ghasemyani S. Promoting AIDS preventive beliefs in Turkmen students by using the health belief model in Aq-Qala. Iran J Health Educ Health Promot 2019; 7(4):323-32. doi: 10.29252/ijhehp.7.4.323.[Persian] [Crossref] [ Google Scholar]
- Mirkarimi K, Charkazi A, Honarvar MR, Kabir MJ, Berdi Ozouni-Davaji R, Aryaie M. Effect of motivational interviewing on physical activity intention among obese and overweight women using protection motivation theory: a randomized clinical trial. Intern Med Today 2016; 22(4):321-7. doi: 10.18869/acadpub.hms.22.4.321.[Persian] [Crossref] [ Google Scholar]
- Baghiani Moghaddam MH, Mohammadi S, Norbala MT, Mazloomi Mahmoudabad SS. The study of factors relevant to skin cancer preventive behavior in female high school students in Yazd based on protection motivation theory. Knowledge and Health 2010;5(1):10-5. [Persian].
- Bai Y, Liu Q, Chen X, Gao Y, Gong H, Tan X. Protection motivation theory in predicting intention to receive cervical cancer screening in rural Chinese women. Psychooncology 2018; 27(2):442-9. doi: 10.1002/pon.4510 [Crossref] [ Google Scholar]
- Dehdari T, Hassani L, Hajizadeh E, Shojaeizadeh D, Nedjat S, Abedini M. Effects of an educational intervention based on the protection motivation theory and implementation intentions on first and second pap test practice in Iran. Asian Pac J Cancer Prev 2014; 15(17):7257-61. doi: 10.7314/apjcp.2014.15.17.7257 [Crossref] [ Google Scholar]
- Orouji MA, Charkazi A, Hazavehei SM, Moazeni M. Practice of motorcycle drivers on helmet use based on health belief model in Khomein city, 2010. Journal of Health and Hygiene 2012;3(2):24-31. [Persian].
- Foster V. Factors Associated with HIV Risky Sexual Behaviors in Older Adults [dissertation]. Georgia State University; 2010.
- Malek Gavgani R, Poursharifi H, Aliasgarzadeh A. Effectiveness of information-motivation and behavioral skill (IMB) model in improving self-care behaviors & Hba1c measure in adults with type2 diabetes in Iran-Tabriz. Procedia Soc Behav Sci 2010; 5:1868-73. doi: 10.1016/j.sbspro.2010.07.380 [Crossref] [ Google Scholar]
- Havaei M, Salehi L, Akbari-Kamrani M, Rahimzadeh M, Esmaelzadeh-Saeieh S. Effect of education based on protection motivation theory on adolescents’ reproductive health self-care: a randomized controlled trial. Int J Adolesc Med Health 2019;33(4). 10.1515/ijamh-2018-0195.
- Khosravi V, Barati M, Moeini B, Mohammadi Y. The effect of an educational intervention based on protection motivation theory on prostate cancer prevention behaviors in men 50 to 75 years old. Hayat 2019;24(4):342-54. [Persian].
- Zarani F, Besharat MA, Sarami G, Sadeghian S. An information-motivation-behavioral skills (IMB) model-based intervention for CABG patients. Int J Behav Med 2012; 19(4):543-9. doi: 10.1007/s12529-011-9193-2 [Crossref] [ Google Scholar]
- Soltani N, Tahmasebi R, Haghighatjoo S, Noroozi A. Effective factors of seat-belt use in front seat passenger on urban trips of Bushehr: application of protection motivation theory. Iran J Health Educ Health Promot 2019; 7(2):220-30. doi: 10.30699/ijhehp.7.2.220.[Persian] [Crossref] [ Google Scholar]
- Shahbazzadeh F, Narimani S, Ahmadi S, Anvari Z. Factors affecting the use of helmets among motorcyclists in Ardabil city 2019. Journal of Safety Promotion and Injury Prevention 2019;7(3):131-7. [Persian].
- Daneshvar F, Barati M, Tapak L, Rezapour Shahkolai F. Factors associated with mothers’ behaviors in injury prevention among premature neonatal in hospital: applying health belief model. J Educ Community Health 2020; 7(2):127-34. doi: 10.29252/jech.7.2.127.[Persian] [Crossref] [ Google Scholar]
- Taheri-Kharameh Z, Bashirian S, Heidarimoghadam R, Poorolajal J, Barati M, Rásky É. Predictors of fall protective behaviors among Iranian community-dwelling older adults: an application of the protection motivation theory. Clin Interv Aging 2020; 15:123-9. doi: 10.2147/cia.s224224 [Crossref] [ Google Scholar]
- Fathi Y, Barati M, Zandiyeh M, Bashirian S. Prediction of preventive behaviors of the needlestick injuries during surgery among operating room personnel: application of the health belief model. Int J Occup Environ Med 2017; 8(4):232-40. doi: 10.15171/ijoem.2017.1051 [Crossref] [ Google Scholar]