J Educ Community Health. 10(1):16-22.
doi: 10.34172/jech.2023.1856
Original Article
The Role of Spirituality and Social Support in Iranian Elderly Happiness: A Cross-sectional Study
Elahe Ezati 1  , Parisa Hosseinikoukamari 2, Mahmood Karimy 2, * , Jordann Rawlins 3, Fatemeh Akbartabar 2, Paria Khalvandi 2
, Parisa Hosseinikoukamari 2, Mahmood Karimy 2, * , Jordann Rawlins 3, Fatemeh Akbartabar 2, Paria Khalvandi 2
Author information:
1Department of Public Health, School of Health, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Public Health, Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran
3Department of Psychology, Department of Health Sciences, University of Rhode Island, USA
Abstract
Background: Spiritual well-being and social support are important factors in reducing loneliness and depression, improving the quality of life, and successful aging in elderly people. This study aimed to investigate the relationship between spiritual well-being, social support, and happiness among elderly people.
Methods: This cross-sectional research was performed on 434 elderly people recruited from the health centers of Saveh University of Medical Sciences in Iran. Eligible participants who matched the selection criteria were selected through a multi-stage random sampling method. Socio-demographic information, the Spiritual Well-Being Scale, social support, and the Oxford Happiness Scale were used as tools for data collection. Finally, all data were analyzed by SPSS, and a multiple linear regression analysis was employed to determine factors associated with happiness.
Results: The mean scores of happiness, spiritual well-being, and social support were 64.0±13.2, 96.4±18.6, and 42.8±10.9, respectively. Overall, 211 (48.6%) elderly people had high levels of spiritual well-being. The findings indicated that 43% (R2=0.43) of the variance of change in happiness could be attributed to spiritual health, social support, and socio-demographic variables, including membership in non-governmental organizations, age, underlying disease status, marital status, and physical activity.
Conclusion: Spiritual well-being and social support play an important role in elderly happiness. The results of the current study might be considered a basis for planning health promotion programs among the elderly. It is recommended that authorities assist in meeting the social and spiritual needs of the elderly to increase their overall happiness.
Keywords: Elderly, Spiritual health, Social support, Happiness
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Ezati E, Hosseinikoukamari P, Karimy M, Rawlins J, Akbartabar F, Khalvandi P. The role of spirituality and social support in Iranian elderly happiness: a cross-sectional study. J Educ Community Health. 2023; 10(1):16-22. doi:10.34172/jech.2023.1856
Introduction
One of the psychological needs of humans is happiness, which has always occupied people’s minds because of its major impact on people’s life (1). Happiness is a positive experience and one of the indicators of mental health resulting from people’s cognitive and emotional evaluation of their life, which has been the focus of many psychologists in the last three decades (2). It is highly important to examine happiness in the elderly because happiness plays an important role in the quality of life and health of the elderly (3). A longitudinal study conducted on more than two thousand Mexican Americans over the age of 65 shows that the amount of positive emotions in people is a predictor of death and illness or disability in participants after 2 years (4).
Due to the rapid increase in elderly individuals, there is a greater demand for society to improve the health, comfort, and well-being of this population. Reduced social connections, physical and mental illness, and loss of relatives create several problems, including low levels of happiness among older individuals (5).
Today, happiness has been emphasized as an important variable of health promotion (3). The research represents that happiness is associated with energy, vitality, movement, and dynamism, and can mitigate the negative effects of stress and positively contribute to physical and mental health (6). Furthermore, evidence demonstrates that there is a significant association between happiness and various components of physical and mental health, including sleep quality, work and social satisfaction, production of stress hormones, and cardiovascular and immune system health (2,3). Due to the relationship between happiness and physical and mental health among the elderly, the World Health Organization has placed great emphasis on happiness as an important component of health and the focus of research seeking to improve overall well-being (7). According to some studies, there is a direct relationship between inner religiosity and spiritual health with positive moods and satisfaction (1-3).
Studies indicate that spiritual well-being is a significant factor in healthy and successful aging. Spirituality has been linked to increased happiness, calmness, and reduced depression in elderly people (8). These findings suggest that elderly people use spirituality and religion to cope with stress and foster peace. The literature on spirituality also demonstrates the positive effect of religious and spiritual practices on coping with chronic diseases, mental well-being, depression, and distress (9). Researchers believe that without spiritual well-being, other physical, mental, and social dimensions may not reach their highest capacity among elderly populations, resulting in lower quality of life (10). On the other hand, Ansari et al reported that spiritual health variables with perceived social support can predict mental well-being. Perceived social support and spiritual health can be effective in promoting health by creating adaptation to the conditions of the elderly. In fact, strengthening the variables of social support in family, friends, and important people, along with paying attention to spiritual health, will improve mental health and happiness (11).
Social support is an essential variable in the quality of life in older people, and a lack of social support is associated with depression and lower levels of happiness. Some studies represented that perceived social support is a contributing factor in effectively coping with stressful life events and conditions (12-14). Furthermore, higher levels of social support, especially familial support, are related to higher life satisfaction and less mental health issues such as depression in older people (3,15). Research indicates that greater social support is linked to better physical functioning and lower mortality rates; therefore, social support is a vital resource in improving the daily lives, happiness, and overall well-being of elderly individuals (12,13).
Due to the global increase in the senior population, there is an increased necessity in improving health and overall well-being for this group; however, there is limited research on the determinants of happiness in older people (16), particularly in developing countries such as Iran (a country with a growing number of the elderly population). Considering the increase in the elderly population in Iran, the need to pay attention to the health issue is extremely necessary to ensure the welfare of this group in society and solve their problems (3,12). Given that only the spiritual health variable has been considered in most studies related to happiness, the present study sought to address this gap in the literature by examining the relationship between happiness and spiritual well-being and social support among elderly people covered by the health centers of Saveh, Iran.
Materials and Methods
Study Population
The present cross-sectional study recruited 448 elderly participants covered by the health centers of Saveh University of Medical Sciences in Iran in 2020. Multi-stage random sampling was used to select participants through a three-step process. First, researchers selected those who met the criteria from all 16 comprehensive health centers in Saveh. Further, all eligible individuals were given a number each and recorded in a list. Finally, 28 individuals who met eligibility criteria (14 males and 14 females) were selected from each health center using the random sampling system and included in the study as the target population. The inclusion criteria were willingness to participate in the study, aged ≥ 60 years, no history of psychotropic drug use, the absence of a first-degree relative with an incurable disease or physical illness, mental or psychological disability, and no factors relating to psychological discomforts such as deaths of relatives or divorce in the past 6 months.
On the other hand, unwillingness to participate in the study, illiteracy, and the presence of an acute illness and mental disorders were the exclusion criteria.
An initial sample size target of 374 was decided based on similar studies of happiness in elderly individuals with an accuracy of 0.05% and a 95% confidence level; however, the sample size was increased to 448 to reach the desired effect size of 1.1 (3,17). All participants were informed about the purpose of the study and confidentiality protocols, and they all gave written informed consent. The questionnaire was completed via self-report by the elderly. If some of the participants were unable to write for any reason, the researcher personally read the questions to them and recorded their answers without any intervention.
Questionnaires
Participants completed several questionnaires to assess background information, happiness, social support, and spiritual well-being.
Background. Questionnaire items assessed socio-demographic characteristics, including age, gender, education, marital status (i.e., divorced, married, and single), insurance status, number of family members, occupation, housing status, physical activity, owning a personal car, and working in a non-governmental organization (NGO).
Happiness. It was measured using the Oxford Happiness Questionnaire. The 29-item measure, based on the Beck Depression Inventory (BDI), uses 4 response options ranging from 0 (completely unhappy) to 3 (completely happy). High (87) and low scores (0) indicate high levels of happiness and unhappiness, respectively. The normal score of the test was in the range of 40-42, and its cut-off point was considered to be 50. Previous studies confirmed the validity and reliability of the Oxford Happiness Questionnaire (17). An examination of the internal consistency of the questionnaire indicated that all 29 items were highly correlated with the total score and had a Cronbach’s alpha of 0.87.
Perceive social support. Social support was determined using the Multidimensional Scale of Perceived Social Support, which is a 12-item tool designed to assess perceived social support in three subscales of friends, family, and important others. In this questionnaire, a 7-point Likert-type scale was used with responses rating 1 (strongly disagree) to 7 (strongly agree). Overall high scores indicate high levels of perceived social support. A previous validation study reported that the measure had high reliability among Iranian populations (α = 0.81) (12), which is in line with the one obtained in the present study (α = 0.82).
Spiritual well-being.It was assessed using the Spiritual Well-Being Scale (Paloutzian & Ellison, 1982), ranging from 1 (strongly disagree) to 6 (strongly agree), in a 20-item questionnaire in which religious health was measured through some questions that were 10 in number, and the other 10 questions measured existential health. Responses and negatively worded questions were scored reversely. Spiritual well-being was classified into low (20-40), moderate (41-99), and high (100-120) levels (18). High overall scores represent high levels of spiritual well-being. The results of the present study demonstrated that the measure had high reliability among the target population (α = 0.83).
Statistical Analyses
The obtained data were analyzed using IBM SPSS, version 22.0. Independent t-tests, one-way analysis of variance, Pearson’s correlation analysis, and multiple linear regression were conducted to determine the association between background variables, happiness, social support, and spiritual well-being among elderly individuals. All methods were performed in accordance with the relevant guidelines and regulations.
Results
Overall, 434 (96.8%) out of 448 participants completed the questionnaires, while 14 cases were excluded due to the incompleteness of the questionnaires. The mean age of the population was 68.7 ± 3.0 years, and 50.9% of the participants were males. Among the participants, 64 (14.8%) and 71 (16.4%) had remarried and were divorced/widowed, respectively. A total of 287 (66%) individuals had underlying health diseases. There was a significant difference between being happy and having a male/female gender, having a personal car, and having a house. Further, there were differences in marital status, age, physical activity, the presence of an underlying illness, and membership in NGO groups (P < 0.05), while no significant difference was found in the level of happiness with the education, remarriage, insurance status, and family dimension (P > 0.05). There was a significant difference between Spiritual well-being and housing, physical activity, marital status, and membership in NGO groups (P < 0.05). Additionally, a significant difference was observed between receiving social support with marital status and membership in NGO groups and having a house and a car, as well as insurance status and remarriage (P < 0.05). Table 1 presents information regarding associations among additional variables.
Table 1.
Association Between Happiness, Spiritual Well-being, Social Report, and Demographic Variables Among Participants
|
Characteristics
|
No. (%)
|
Spiritual Well Being
|
Social Support
|
Happiness
|
|
Mean±SD
|
P
-value
|
Mean±SD
|
P
-value
|
Mean±SD
|
P
-value
|
| Gender |
|
|
|
|
|
|
|
| Male |
221 (50.9) |
95.4 ± 18.9 |
0.32 |
43.3 ± 6.8 |
0.46 |
65.7 ± 13.8 |
0.01 |
| Female |
213 (49.1) |
98.1 ± 18.1 |
42.1 ± 12.0 |
60.9 ± 11.7 |
| Remarriage |
|
|
|
|
|
|
|
| Yes |
64 (14.8) |
97.6 ± 15.7 |
0.4 |
43.1 ± 9.2 |
0.001 |
65.8 ± 11.8 |
0.04 |
| No |
370 (85.2) |
96.1 ± 19.0 |
37.4 ± 11.2 |
60.1 ± 12.6 |
| Insurance status |
|
|
|
|
|
|
|
| Yes |
396 (91.2) |
98.2 ± 17.6 |
0.39 |
45.1 ± 10.8 |
0.01 |
64.4 ± 13.3 |
0.16 |
| No |
38 (8.8) |
96.8 ± 16.5 |
40.5 ± 12.2 |
60.3 ± 12.8 |
| Housing status |
|
|
|
|
|
|
|
| Personal |
395 (91) |
97.7 ± 17.9 |
0.007 |
43.2 ± 10.7 |
0.01 |
64.6 ± 13.2 |
0.04 |
| tenant |
39 (9) |
86.6 ± 21.0 |
38.4 ± 12.4 |
58.2 ± 11.9 |
| Car |
|
|
|
|
|
|
|
| Yes |
115 (26.5) |
97.9 ± 17.3 |
0.48 |
45.8 ± 10.4 |
0.02 |
67.7 ± 12.0 |
0.01 |
| No |
319 (73.5) |
95.8 ± 19.0 |
41.8 ± 10.9 |
62.7 ± 13.4 |
| Underlying diseases |
|
|
|
|
|
|
|
| Yes |
287 (66) |
96.0 ± 19.3 |
0.71 |
42.6 ± 11.0 |
0.8 |
59.7 ± 13.8 |
0.01 |
| No |
147 (34) |
97.1 ± 17.2 |
43.0 ± 10.9 |
64.4 ± 14.1 |
| Exercise |
|
|
|
|
|
|
|
| Yes |
161 (37) |
99.6 ± 17.5 |
0.01 |
43.6 ± 11.1 |
0.29 |
67.5 ± 12.7 |
0.001 |
| No |
273 (63) |
93.4 ± 19.1 |
42.0 ± 10.8 |
60.4 ± 12.9 |
| Social groups (NGO) |
|
|
|
|
|
|
|
| Yes |
150 (34.6) |
99.8 ± 16.9 |
0.004 |
46.9 ± 10.9 |
0.001 |
67.6 ± 12.5 |
0.002 |
| No |
284 (65.4) |
92.6 ± 18.9 |
37.6 ± 11.8 |
61.7 ± 13.3 |
| Family dimension |
|
|
|
|
|
|
|
| < 3 |
235 (54.2) |
96.4 ± 18.8 |
0.77 |
44.0 ± 10.3 |
0.07 |
65.1 ± 14.0 |
0.14 |
| ≥ 3 |
199 (45.8) |
96.2 ± 18.9 |
41.1 ± 12.1 |
62.3 ± 12.2 |
| Marital status |
|
|
|
|
|
|
|
| Married |
363 (83.6) |
97.8 ± 17.9 |
0.01 |
43.6 ± 10.1 |
0.02 |
65.3 ± 13.2 |
0.001 |
| Divorced or widowed |
71 (16.4) |
89.3 ± 20.4 |
38.8 ± 13.8 |
57.0 ± 11.1 |
| Education |
|
|
|
|
|
|
|
| Illiteracy or elementary school |
246 (56.6) |
94.3 ± 17.5 |
0.63 |
41.9 ± 10.8 |
0.7 |
67.5 ± 13.6 |
0.78 |
| Secondary |
163 (37.5) |
96.3 ± 18.4 |
42.5 ± 10.3 |
66.2 ± 14.4 |
| university |
25 (5.8) |
94.6 ± 18.6 |
42.6 ± 12.3 |
67.8 ± 14.1 |
| Age (y) |
|
|
|
|
|
|
|
| 60-69 |
252 (58) |
96.7 ± 18.6 |
0.3 |
44.0 ± 9.5 |
0.14 |
67.4 ± 12.8 |
0.03 |
| 70-79 |
135 (31) |
94.2 ± 17.4 |
42.9 ± 11.4 |
63.6 ± 12.7 |
| 80 ≥ |
47 (11) |
96.4 ± 19.2 |
38.6 ± 11.8 |
60.1 ± 11.2 |
Note. SD: Standard deviation; NGO: Non-governmental organization.
Based on data in Table 2, the mean scores of happiness, spiritual well-being, and social support were 64.0 ± 13.2, 96.4 ± 18.6, and 42.8 ± 10.9, respectively. The results of the Pearson correlation test indicated a direct and significant relationship between spiritual well-being and happiness (r = 0.51, P < 0.01), social support and happiness (r = 0.47, P < 0.01), social support and spiritual well-being (r = 0.38, P < 0.01), and family dimension and social support (r = 0.13, P < 0.01) while a negative correlation between age and happiness (r = - 0.27, P < 0.01).
Table 2.
The Correlation Coefficients for Happiness, Spiritual Well-being, Social Support, and Demographic Variables Among Participants
|
Variable
|
1
|
2
|
3
|
4
|
5
|
Mean±SD
|
Range of Scores
|
| 1. Happiness |
1 |
|
|
|
|
64.0 ± 13.2 |
0-87 |
| 2. Spiritual well-being |
0.51** |
1 |
|
|
|
96.4 ± 18.6 |
20-120 |
| 3. Social support |
0.47** |
0.38** |
1 |
|
|
42.8 ± 10.9 |
0-72 |
| 4. Age |
-0.27** |
-0.11 |
-0.06 |
1 |
|
68.7 ± 3.0 |
60 ≥ |
| 5. Family dimension |
-0.09 |
0.1 |
0.13** |
0.09 |
1 |
3.1 ± 1.5 |
1-12 |
Note. SD: Standard deviation.
Figure 1 illustrates the level of spiritual well-being among the participants. Overall, 211 out of 434 and 205 participants reported high (score of 100-120) and moderate (41-99) levels of spiritual well-being, respectively.
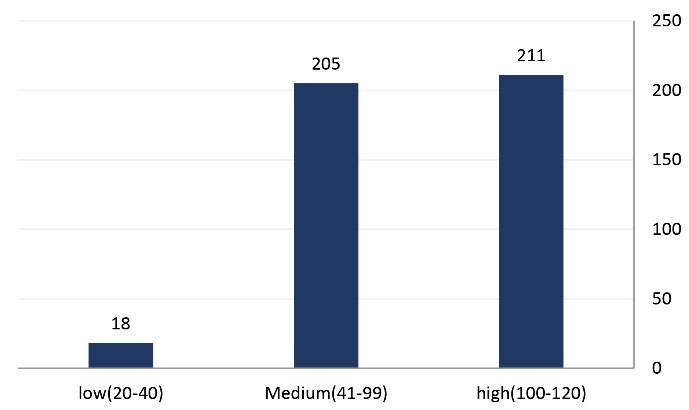
Figure 1.
Frequency of Spiritual Well-being Status Among Participants
.
Frequency of Spiritual Well-being Status Among Participants
Multiple linear regressions were conducted using happiness, social support, spiritual health, and demographic variables. The findings revealed that spiritual well-being (β = 0.30, P < 0.01), physical activity (β = 0.28, P < 0.01), social support (β = 0.27, P < 0.01), and age (β = -0.26, P < 0.01) significantly predicted happiness (Table 3). The results indicated that 43% of the variance of happiness could be attributed to spiritual health, social support, and variables such as membership in NGOs, age, underlying disease status, marital status, and physical activity (R2 = 0.43). Based on the results, there was a significant relationship between happiness, spiritual well-being, and social support when controlling for age and marital status (Table 3).
Table 3.
Multiple Linear Regression for Association’s Happiness Between Social Support, Spiritual Well-being, and Demographic Variables Among Participants
|
Model
|
Unstandardized Coefficients
|
Standardized Coefficients
|
t
|
P
Value
|
95.0% Confidence Interval for B
|
Adjusted R Square
|
|
B
|
Std. Error
|
Beta
|
Lower Bound
|
Upper Bound
|
| Social support |
0.19 |
0.04 |
0.27 |
4.6 |
0.001 |
0.11 |
0.28 |
|
| Spiritual well-being |
3.43 |
0.93 |
0.3 |
3.6 |
0.001 |
1.6 |
5.2 |
|
| Age |
-7.39 |
1.99 |
-0.26 |
-3.7 |
0.001 |
-11.3 |
-3.4 |
0.43 |
| Non-governmental organization group (reference category: No) |
2.57 |
1.03 |
0.18 |
2.4 |
0.01 |
0.53 |
4.6 |
|
| Marriage (reference category: Divorced or widowed) |
0.19 |
0.09 |
0.15 |
1.9 |
0.04 |
0.03 |
0.38 |
|
| Underlying diseases (reference category: No) |
-4.7 |
1.48 |
-0.17 |
-3.2 |
0.002 |
-7.7 |
-1.8 |
|
| Exercise (reference category: No) |
0.33 |
0.12 |
0.28 |
2.6 |
0.008 |
0.08 |
0.58 |
|
Discussion
This study assessed the association between spiritual well-being, happiness, and social support in elderly people. The results of the present study showed that spiritual well-being was the most important predictor of happiness, and roughly half of the sample (48.6%) had high spiritual well-being scores. This relationship between spiritual well-being and happiness is supported by the current literature (19,20). The finding of one study demonstrated that spiritual well-being could be a useful resource in improving the happiness of older people (21). In a similar study, spiritual well-being predicted 35% of the variance of happiness (22), further indicating the important role of spirituality in promoting happiness among elderly individuals. According to the results of our study and previous studies (23,24), acting on religious beliefs strengthens the spiritual relationship with God and improves meaning-finding in one’s life, which increases reported happiness. A possible explanation for these findings is that religious people often choose their closest friends among their religious affiliations, religion values positive outlook, and kindness to others which can generally increase happiness.
The results of the present study demonstrated that physical activity was a significant predictor of happiness. Our findings are consistent with those of previous studies, indicating that happiness was higher for active elderly individuals than for inactive elderly (12,25). This same study examined the health status of participants and represented that regular exercise increased the physical and mental performance of the sample (26). Similarly, researchers found that among older people who exercised and had no underlying diseases, there was less reported depression (27). The literature and our current findings suggest that physical activity is integral in achieving and maintaining happiness and physical health among elderly people (28). Furthermore, the findings suggest that physical activity impacts important components of happiness, including greater job success, work satisfaction, social interactions, improvements in physical health, and self-confidence (29).
In the current study, social support and membership in NGOs were predictors of happiness. Consistent with our findings, Lu (30) and Moeini et al (3) found that social support and membership in social groups were also strong predictors of happiness. Some studies (13,31) showed that social support is an important item in maintaining and promoting physical and cognitive health in older people, and it was further revealed that having social support positively could affect their daily life (e.g., participants reported feeling refreshed). These findings, in addition to the literature, suggest that belonging to social groups can increase self-confidence, self-efficacy, and self-esteem in individuals. This impact is important because self-confidence and self-esteem are associated with overall life satisfaction and thus happiness. Considering that loneliness and isolation are potential health threats to old age, it is necessary for society to promote supportive environments and empowerment of the elderly to establish and utilize social support more robustly.
The results indicated that happiness was higher in married elderly individuals and men and was inversely related to aging such that as age increased, happiness represented a decrease. The findings also indicate that there is an essential relationship between happiness and underlying diseases, car ownership, and housing ownership. In line with these findings, researchers concluded that health-related factors and the absence of disease not only affected self-reported happiness but were also affected by happiness (32). Furthermore, studies examining the prevalence of successful aging in the United States reported that male gender and social and economic status were significantly associated with successful aging and happiness (33). The literature also posits that marriage is an important factor in happiness among East Asian countries (34). This evidence supports the economic theory that low income meant low levels of happiness as reported earlier (35).
One of the strengths of this study was the investigation and analysis of several important variables related to happiness in the elderly. In addition, three standard questionnaires with different questions were used in the current study compared to other studies. On the other hand, a limitation of the present study was the physical weakness of elderly participants and their early fatigue, which could influence the study data. Additionally, hearing impairments are common among elderly populations, which resulted in questions needing to be explained numerous times. This may have caused confusion or lack of an understanding of items within the questionnaires; however, the recruiting researcher decreased the bias in data collection. The cross-sectional nature of the study makes it challenging to derive causal relationships from the cross-sectional analysis.
Conclusion
According to the results of the present study, there was a significant relationship between spiritual well-being, social support, and happiness in older people; therefore, it appears that spiritual well-being, along with factors such as membership in social groups and economic support, can increase happiness in older people, and in turn, contribute to a higher quality of life among elderly. The results of our study provide insights for planning health promotion programs among the elderly. It is recommended that authorities assist in meeting the social and spiritual needs of the elderly to increase their overall happiness.
Acknowledgements
The authors would like to thank all the elderly people; the present study would not have been completed without their contribution.
Authors’ Contribution
Conceptualization: Elahe Ezati.
Data curation: Fatemeh Akbartabar, Paria Khalvandi.
Formal analysis: Mahmood Karimy.
Funding acquisition: Parisa Hosseinikoukamari, Mahmood Karimy.
Investigation: Fatemeh Akbartabar, Paria Khalvandi.
Methodology: Parisa Hosseinikoukamari, Mahmood Karimy.
Project administration: Mahmood Karimy.
Resources: Parisa Hosseinikoukamari, Mahmood Karimy.
Supervision: Mahmood Karimy.
Validation: Jordann Rawlins.
Visualization: Elahe Ezati.
Writing—original draft: Mahmood Karimy.
Writing—review and editing: Jordann Rawlins, Elahe Ezati.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
The study was approved by the Institutional Review Board and the Ethics Committee of Saveh University of Medical Sciences, Saveh, Iran (approval code: IR.SAVEHUMS.REC.1398.022). Furthermore, all participants in this study completed a written informed consent form. All methods were performed in accordance with the relevant guidelines and regulations (e.g., the Declaration of Helsinki).
Funding
This study was supported by funding from the Saveh University of Medical Sciences (grant no. 990423).
References
- Hedayat F, Sadegzade S. Meta-analysis of the relationship between spiritual intelligence with happiness. New Approach in Educational Sciences 2020; 2(1):59-68. doi: 10.22034/naes.2020.228237.1030.[Persian] [Crossref] [ Google Scholar]
- Moeini B, Rezapur-Shahkolai F, Tapak L, Geravandi A, Parsamajd S. Relationship between happiness and mental health with social capital among health workers. J Educ Community Health 2020; 7(2):119-25. doi: 10.29252/jech.7.2.119 [Crossref] [ Google Scholar]
- Moeini B, Barati M, Farhadian M, Heydari Ara M. The association between social support and happiness among elderly in Iran. Korean J Fam Med 2018; 39(4):260-5. doi: 10.4082/kjfm.17.0121 [Crossref] [ Google Scholar]
- Carr A. Positive Psychology: The Science of Happiness and Human Strengths. Routledge; 2013.
- Abdian T, Banaee E, Ramezanli S. The effectiveness of positive psychology of happiness and hopefulness of elderly people in elderly care centers. J Gerontol 2021;6(2):1-9. [Persian].
- Syed Elias SM, Neville C, Scott T. The effectiveness of group reminiscence therapy for loneliness, anxiety and depression in older adults in long-term care: a systematic review. Geriatr Nurs 2015; 36(5):372-80. doi: 10.1016/j.gerinurse.2015.05.004 [Crossref] [ Google Scholar]
- Changizi F, Panahali A. Effectiveness of group narrative therapy on life expectancy and happiness of the elderly in Tabriz. Journal of Instruction and Evaluation 2016;9(34):63-76. [Persian].
- Garssen B, Visser A, Pool G. Does spirituality or religion positively affect mental health? Meta-analysis of longitudinal studies. Int J Psychol Relig 2021; 31(1):4-20. doi: 10.1080/10508619.2020.1729570 [Crossref] [ Google Scholar]
- Emlet CA, Harris L, Pierpaoli CM, Furlotte C. “The journey i have been through”: the role of religion and spirituality in aging well among HIV-positive older adults. Res Aging 2018; 40(3):257-80. doi: 10.1177/0164027517697115 [Crossref] [ Google Scholar]
- Zareipour M, Khazir Z, Valizadeh R, Mahmoodi H, Ghelichi Ghojogh M. The association between spiritual health and blood sugar control in elderly patients with type 2 diabetes. Elder Health J 2016;2(2):67-72. [Persian].
- Ansari O, Shafipour V, Heidari Gorji MA, Mohammadpour RA. Association between subjective wellbeing and perceived social support and spiritual well-being in hemodialysis patients. J Mazandaran Univ Med Sci 2018;28(166):140-50. [Persian].
- Zareban I, Araban M, Rohani MR, Karimy M, Zamani-Alavijeh F, Babanejad M. High blood pressure self-care among hypertensive patients in Iran: a theory-driven study. J Hum Hypertens 2022; 36(5):445-52. doi: 10.1038/s41371-020-00429-9 [Crossref] [ Google Scholar]
- Taher M, Abredari H, Karimy M, Abedi A, Shamsizadeh M. The relation between social support and adherence to the treatment of hypertension. J Educ Community Health 2014; 1(3):63-9. doi: 10.20286/jech-010348 [Crossref] [ Google Scholar]
- Arabshahi A, Gharlipour Z, Mohammadbeigi A, Mohebi S. Effect of educational intervention based on social support received by the spouse on promoting adherence to treatment regimen in hypertensive patients. J Educ Community Health 2020; 7(3):153-60. doi: 10.29252/jech.7.3.153 [Crossref] [ Google Scholar]
- Tengku Mohd TAM, Yunus RM, Hairi F, Hairi NN, Choo WY. Social support and depression among community dwelling older adults in Asia: a systematic review. BMJ Open 2019; 9(7):e026667. doi: 10.1136/bmjopen-2018-026667 [Crossref] [ Google Scholar]
- Steptoe A. Investing in happiness: the gerontological perspective. Gerontology 2019; 65(6):634-9. doi: 10.1159/000501124 [Crossref] [ Google Scholar]
- Alipour A, Agah Heris M. Reliability and validity of the Oxford Happiness Inventory among Iranians. Journal of Iranian Psychologists 2007;3(12):287-98. [Persian].
- Ellison CW. Spiritual well-being: conceptualization and measurement. J Psychol Theol 1983; 11(4):330-8. doi: 10.1177/009164718301100406 [Crossref] [ Google Scholar]
- Sharma SK, Sharma OP. Spirituality leads to happiness: a correlative study. Int J Indian Psychol 2016; 3(2):50-4. doi: 10.25215/0302.177 [Crossref] [ Google Scholar]
- Thauvoye E, Vanhooren S, Vandenhoeck A, Dezutter J. Spirituality and well-being in old age: exploring the dimensions of spirituality in relation to late-life functioning. J Relig Health 2018; 57(6):2167-81. doi: 10.1007/s10943-017-0515-9 [Crossref] [ Google Scholar]
- Khodarahimi S, Ghadampour E, Karami A. The roles of spiritual well-being and tolerance of uncertainty in prediction of happiness in elderly. An Psicol 2021; 37(2):371-7. doi: 10.6018/analesps.446871 [Crossref] [ Google Scholar]
- Choudhari S, Singh BG. Spiritual practice and happiness among elder. IAHRW Int J Soc Sci 2019; 7(5-I):1127-30. [ Google Scholar]
- Hsiao YC, Chiang HY, Chien LY. An exploration of the status of spiritual health among nursing students in Taiwan. Nurse Educ Today 2010; 30(5):386-92. doi: 10.1016/j.nedt.2009.05.001 [Crossref] [ Google Scholar]
- Wallace JM. The Contributions of Spirituality and Religious Practices to Children’s Happiness [dissertation]. University of British Columbia; 2010.
- Shah SA, Safian N, Ahmad S, Wan Ibadullah WAH, Mohammad ZB, Nurumal SR. Factors associated with happiness among Malaysian elderly. Int J Environ Res Public Health 2021; 18(7):3831. doi: 10.3390/ijerph18073831 [Crossref] [ Google Scholar]
- Grant S, Todd K, Aitchison TC, Kelly P, Stoddart D. The effects of a 12-week group exercise programme on physiological and psychological variables and function in overweight women. Public Health 2004; 118(1):31-42. doi: 10.1016/s0033-3506(03)00131-8 [Crossref] [ Google Scholar]
- Eyigor S, Karapolat H, Durmaz B. Effects of a group-based exercise program on the physical performance, muscle strength and quality of life in older women. Arch Gerontol Geriatr 2007; 45(3):259-71. doi: 10.1016/j.archger.2006.12.001 [Crossref] [ Google Scholar]
- Fortier MS, Morgan TL. How optimism and physical activity interplay to promote happiness. Curr Psychol 2022; 41(12):8559-67. doi: 10.1007/s12144-020-01294-y [Crossref] [ Google Scholar]
- Lin YT, Chen M, Ho CC, Lee TS. Relationships among leisure physical activity, sedentary lifestyle, physical fitness, and happiness in adults 65 years or older in Taiwan. Int J Environ Res Public Health 2020; 17(14):5235. doi: 10.3390/ijerph17145235 [Crossref] [ Google Scholar]
- Lu L. Social support, reciprocity, and well-being. J Soc Psychol 1997; 137(5):618-28. doi: 10.1080/00224549709595483 [Crossref] [ Google Scholar]
- Jokar F, Asadollahi AR, Kaveh MH, Ghahramani L, Nazari M. Relationship of perceived social support with the activities of daily living in older adults living in rural communities in Iran. Iran J Ageing 2020; 15(3):350-65. doi: 10.32598/sija.10.15.3.2773.2.[Persian] [Crossref] [ Google Scholar]
- Graham C. Happiness and health: lessons--and questions--for public policy. Health Aff (Millwood) 2008; 27(1):72-87. doi: 10.1377/hlthaff.27.1.72 [Crossref] [ Google Scholar]
- McLaughlin SJ, Connell CM, Heeringa SG, Li LW, Roberts JS. Successful aging in the United States: prevalence estimates from a national sample of older adults. J Gerontol B Psychol Sci Soc Sci 2010; 65B(2):216-26. doi: 10.1093/geronb/gbp101 [Crossref] [ Google Scholar]
- Hori M, Kamo Y. Gender differences in happiness: the effects of marriage, social roles, and social support in East Asia. Appl Res Qual Life 2018; 13(4):839-57. doi: 10.1007/s11482-017-9559-y [Crossref] [ Google Scholar]
- Napa W, Granger J, Kejkornkaew S, Phuagsachart P. Family happiness among people in a Southeast Asian city: grounded theory study. Nurs Health Sci 2020; 22(2):292-9. doi: 10.1111/nhs.12688 [Crossref] [ Google Scholar]