J Educ Community Health. 10(1):49-57.
doi: 10.34172/jech.2023.1982
Systematic Review Articles
Systematic Review of Health Literacy and Health Promotion in School-Aged Adolescents
Shanti Prasad Khanal 1, *  , Chitra Bahadur Budhathoki 1, Orkan Okan 2, Edwin van Teijlingen 3, Mohan Kumar Sharma 4, Jib Acharya 5, Cate Wood 6
, Chitra Bahadur Budhathoki 1, Orkan Okan 2, Edwin van Teijlingen 3, Mohan Kumar Sharma 4, Jib Acharya 5, Cate Wood 6
Author information:
1Faculty of Education, Tribhuvan University, Nepal
2Technical University Munich, Department of Sport and Health Sciences, Munich, Germany
3Bournemouth University, United Kingdom
4Graduate School of Education, Tribhuvan University, Nepal
5ANC Premium Services Ltd/Bournemouth University, United Kingdom
6Department of Nursing, Faculty of Health & Life Sciences, Oxford Brooks University, United Kingdom
Abstract
Background: The literature has identified gaps in adolescent health literacy (AHL) measurements, as well as how the health literacy (HL) level is related to health promotion (HP) aspects. This study aimed to examine the tools used to measure HL and determine its relation with HP among adolescents.
Methods: Three online databases (HINARI, PubMed, and DOAJ) were searched to conduct a systematic assessment of papers published between January 1, 2016, and January 1, 2021. In this review, 373 articles were identified from these databases. After removing duplicates and screening titles and abstracts of articles, 49 full texts were selected for full-text reading. After comprehensive reading, 23 papers were appraised for qualitative synthesis.
Results: Of the 23 reviewed papers, 21 focused on assessing AHL measures, and 15 addressed the association between AHL and HP. Seven studies used the HL School-Aged Children instrument. The findings suggested that the methodological and conceptual underpinnings of HL measures are insufficient. Furthermore, HL acts as an independent and positive mediator for many facets of HP.
Conclusion: This review offers a warning to practitioners and educationists interested in measuring HL as the number of measurement tools is quite huge with different tools applying different scales.
Keywords: Health literacy, Measures, Health promotion, School-aged adolescents
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Khanal SP, Budhathoki CB, Okan O, van Teijlingen E, Sharma MK, Acharya J, et al. Systematic review of health literacy and health promotion in school-aged adolescents. J Educ Community Health. 2023; 10(1):49-57. doi:10.34172/jech.2023.1982
Introduction
The term health literacy (HL)was developed in conjunction with health education in 1974 by Simonds (1) and has recently gained popularity (2,3). In addition, it is an outcome of health education, learning (4-6), culture, language, and health services (2), which is why many scholars place HL into the wider school context (7). HL is recognized as a key element of the sustainable development goal with substantial public health benefits (8), as well as a health promotion (HP) planning tool (9). There is a significant and positive relationship between HL, health behavior (10), health outcomes, health costs (11),chronic disease, health information demands, and equity (12).
In the past, the concept of HL referred to an individual’s capacity to obtain, process, and comprehend health information (9) to make decisions about healthcare, disease prevention, andHP(13). Moreover, it is a multidimensional concept that includes functional, interactive, and, critical competencies (14), multi-level determinants (13), and empowerment (12). There are various definitions of adolescent health literacy(AHL). A systematic review by Bröder et al identified 12 definitions and 21 models of HL (15). It demonstrated many definitions and models for young or middle school students. The researchers defined HL as how children and adolescents receive, understand, evaluate, communicate, and use health information (15-18).
HL has various measurement scales, most of which have been used for adults (19,20). Further, few scales are employed to test cognitive and literacy skills for health from the perspectives of HP, education, or public health (8). Only a few scales and studies have focused on young people. A review paper published in 2018 identified 15 generic HL tools for children and adolescents. Of these, seven cases were functional and subjective HL instruments (16). Guo et al conducted a review and found 29 HL instruments, among which functional HL (FHL) comprises half (21). Likewise, Ormshaw et al concluded that the majority (n = 14) assessed HL directly using an objective measure (22). All three studies lacked the quality assessment of studies included with these reviews nor did they cover the relationship between HL and the HP of adolescents. Therefore, it is uncertain which instrument is the most valid, reliable, and practical for use with adolescents.
To address these gaps in understanding, this systematic review has addressed two research questions (RQ), including what instruments are used to measure HL among school-based adolescents and how the HL and HP of adolescents are related to each other. The first part of this review analyses the major characteristics of HL measures, including place of operation, the types of scale/score, method of assessment, competencies, reliability, the time of administration, methodology, and AHL situation. Similarly, the relationship of the HL with aspects of the HP is analyzed in the second part of the review. Our review of the literature was conducted to rigorously analyze all papers published between 2016 and 2021 to gain a better understanding of the literature. In our opinion, this study may have filled in some gaps in the measurement, research methodology, and how HL is related to HP. In addition, it will provide an opportunity for academics who are interested in collecting and assessing data or using them appropriately.
Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (23) to ensure a high level of evidence. The PRISMA flow diagram (24) highlights the method of finding and incorporates the relevant articles (16,17).
Data Source and Searching Strategies
This study was performed using three online databases (HINARI, PubMed, and Directory of Open Access Journals) which published the articles between January 1, 2016, and January 1, 2021. Boolean operators (AND/OR) were applied to combine search words around adolescence (including young people and teenagers), HL/HP, and relationship/association.
Adolescent OR school adolescent OR school teen health literacy AND health promotion were used as key search terms. The first searched term was “adolescent OR school teen health literacy”, and the second term was “relationship” OR “correlation” OR “association” with health promotion. Three databases used the following algorithm:
{((TitleCombined: (adolescent)) OR (TitleCombined: (school adolescent)) OR (school teen health literacy)) AND (relationship OR Correlation OR Association with health promotion)}
Eligibility Criteria
First, all authors contributed to the formulation of the eligibility criteria. The applied eligible criteria are provided in Table 1.
Table 1.
Eligible Criteria
|
Category
|
Eligible
|
Not Eligible
|
| Population |
Included school adolescents aged between 10 and 18 from any setting and any country. |
Age below 10 or over 18 |
| Intervention |
Included evaluation and screening of generic HL situations and implementation of educational interventions to increase access, understanding, accounting, and use of health information in at least one aspect of HP was included. |
Interventions that did not emphasize HL through education, HP, or public health. |
| Context |
Included school setting studies along with any research designs studies related to generic HL. |
Domain-specific studies |
| Outcome |
Aimed to measure the HL level, a psychosomatic test of measures, examine at least one aspect of HP, and analyze it with the relationship between HL an HP |
Only one outcome of interest was not even included. |
| Study design |
Included original paper published in English and in a peer-review study. |
Any other language and non-peer-reviewed papers and other book chapters, case studies, protocol papers, and the like. |
Note. HR: Health literacy; HP: Health promotion.
Screening, Data Extraction, and Analysis
Two separate authors (SPK and CBB) performed the search. Moreover, SPK and JA scanned the title and abstracts for relevance. Further, SPK, JA, and MKS performed the full-text analysis. In addition, SPK and CW independently checked the result, while OO and EvT assessed the results to reach a consensus around the included studies. References were imported into the electronic database software tool (EndNote X9). Information identified in the relevant publications related to the measures of an HL level and the association between their HL level and HP of school adolescents were independently extracted by SPK and MKS.
The data were extracted from papers based on the characteristics of the included studies (e.g., the first author, publication year, and country, general characteristics of the instruments, psychometric properties, and relationships between HL and HP).
Each author separately evaluated papers for qualifying in accordance with the criteria to reduce the selection bias. To compare their findings, resolve any disagreements, and determine whether each article should be incorporated, we convened a group meeting. The study team considered contrary views and then concluded by consensus.
The data were collected and summarized for each paper, and then the summaries were tabulated by themes, including information such as the name of the author(s), year of publication, type, components, items, and mode of administration of measures, HL level, psychometric properties, and sample size.
The review of the literature yielded 373 articles (Figure 1). A total of 278 articles were removed after identifying duplicates, and 44 articles were screened and reviewed for abstracts. Additionally, 49 articles were retrieved for full-text reviews. Next, 26 articles were excluded after reviewing the full text. Finally, 23 full-text articles were reviewed based on 373 database searches.
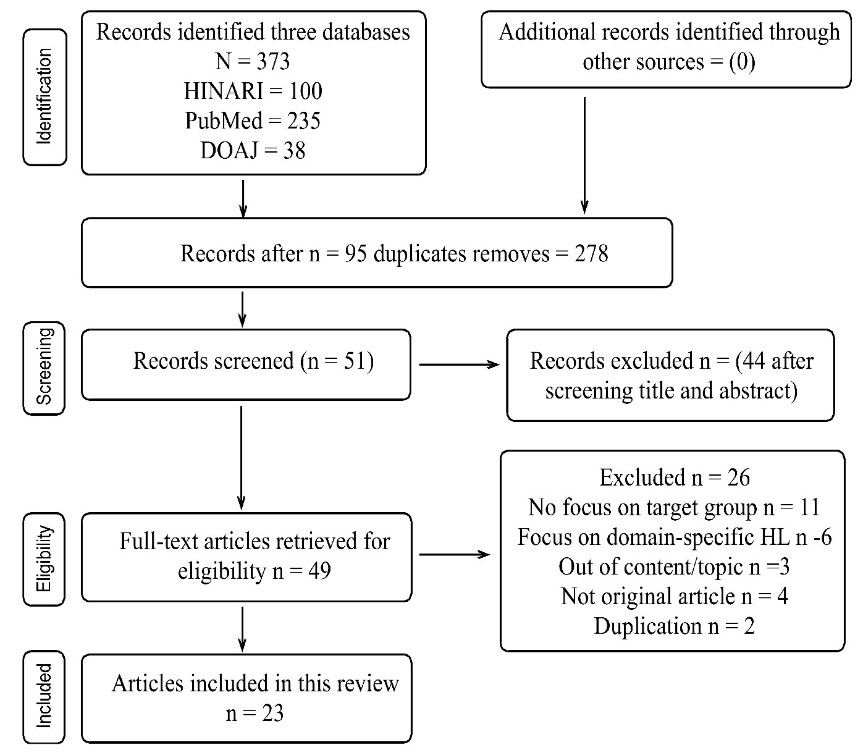
Figure 1.
PRISMA Chart for a Systematic Review. Note. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-analyses.
.
PRISMA Chart for a Systematic Review. Note. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Results
The review of the literature yielded 373 articles (Figure 1). Overall, 278 articles were removed after identifying duplicates, and a total of 44 articles were screened and reviewed for abstracts, and 49 articles were retrieved for full-text reviews. After reviewing the full text, 26 articles were excluded, and finally, 23 full-text articles were reviewed according to 373 database searches. Among the selected papers, 21 papers were assessed for research question 1 such as measures and the AHL level, and 15 papers described its relationship/association with HP (research question 2).
Health Literacy Measures and Level of Adolescent Health Literacy
HL Measure
In total, 21 identified papers were suitable in 13 of these different measures and were identified to assess AHL. Based on data in Table S1, four instruments (25-28) are new, and nine scales already existed or were adapted. Only three HL scales of Health Literacy Scale- European Union (HLS-EU), Functional Health Literacy (FHLs), and HLS for Japanese adults had been initially developed for adults. The other ten were specially developed for adolescents. Seven papers (29-35) used HL among School-Aged Children (HLSAC) scale. Three and two studies used Newest Vital Sign (NVS) (36-38) and Chinese Adolescent Interactive HL Questionnaire (CAIHLO) (39,40), respectively. However, other studies employed a different scale such as HLS-EU (25), an HLS for Thai children who were overweight (41), an HLS developed by Ran (26), the Rapid Estimate of Adolescent Literacy in Medicine Teen (REALM teen) measure (27), an HL screening instrument developed by Chew et al (42), pre-test and post-test tools (43), theHL Assessment Scale for Adolescents into Arabic Language (HAS-A-AR) (44), the FHLs (45), and HL Measure for Adolescent (HELMA) (28).
Countries of Developed and Setting
Three of the HL scales (i.e., NVS, fun-HLS, HL Screening Instrument, and REALM-Teen [pre-test and post-test]) were developed and used in the United States, followed by three from China (i.e., subjective HL scale and CAIHLO). There was one copy from Finland (HLSAC), Europe, Thailand, Palestine, Japan, and Iran. All studies were conducted in a school setting. Three (32,38,42), six (26,35,36,39,40,43), and two (39,40) studies were conducted in senior, junior, and both junior and senior high schools, respectively. The remaining studies did not mention the schooling level of participants. Similarly, looking at the children’s age group, six (28,29,31,33,34,38) and three (30,37,42) studies focused on 10-14 and 15-19 years old, respectively, and only five studies (25,27,32,44,45) used 11-19 years adolescents. The remaining studies mentioned no age group.
Overall, six measures and 15 studies were based upon subjective HL, and only five measures and six studies (27,30,32,34,42,45) employed objective/functional measures of HL. One study utilized one subjective and one objective scale (45). The studies were conducted in 26 different countries. Among them, two studies (33,34) were performed cross-national, and others were conducted at the national level. Five (32,27,36,42,43), three (26,33,40), two (29,31), and two (28,38) studies were performed in the USA, China, Finland, and Iran, respectively. One study was conducted in Norway (30), Thailand (41), Australia (25), Turkey (35), Palestine (44), Japan (45), Pakistan (37), and the like.
Methodological Characteristics
In the context of psychometric properties, six studies (27,31,37,42,43,45) did not provide reliability and validity on their instruments. Others reported the reliability of the instruments. Among these, the scales of nine studies had a strong ( > 0.85) value of reliability, and four studies had good reliability. Only one instrument (41) had a weak value ( < 0.70) of reliability. Seven studies did not have well-described psychometric properties and did not mention a reliability value. One study (25) mentioned the validity of the instrument.
Regarding sampling design and size in this review, only 13 papers mentioned the sampling design. Of those, there was greater use of a multi-stage sample (n = 5) (26,28,37,39,40) and cluster (n = 3) (25,32,38). Similarly, four studies used convenience (36,45) and stratified (41,44) sampling methods, and one study employed a snowball (30) sampling method. In the remaining seven reviewed papers (27,29,31,33,35,42,43), the sampling method was not reported at all. With regard to the sample size of the included studies, fourteen studies were conducted using large sample sizes. Only seven studies (27,28,36-38,42,45) had a small sample size. The participants of the combined study were 11-19-year-old students studying at 7-12th levels of the school and were the most common groups (Table S1).
Situation of Adolescent Health Literacy
The eight reviewed studies conducted in Thailand (41), China (26), Belgium (33), Czechia (34), Turkey (35), Texas (36), Pakistan (37), and Iran (38) reported that the HL level of the school adolescents was inadequate/marginal. Six studies reported a moderate level of HL. Some papers had not cleared the HL situation of adolescents. There were large percentages of adolescents with inadequate HL in each nation. Several systematic review papers reported the same finding of the high prevalence of adequate HL among adolescents and youths (15,16,46). Eight studies demonstrated a statistically significant correlation between age, parental education, membership in the sports club, ethnic group, gender, grade, medication, older adolescents, countries, and AHL level. In another study, it was found that the perceived critical HL and perceived FHL were not directly related. Hence, the HL level of adolescents is determined by different factors (Table S1).
Health Literacy Level and Health Promotion of School-aged Adolescents
Fifteen studies reviewed the relationship of HL with 22 components of HP. Health behavior was included in eight studies (25,27,29-31,38,40,41) and showed that some health behaviors were statistically significantly associated with HL. For example, HL is an independent factor/mediator (1) for increasing HP behavior such as hand-washing (30), healthy food (29,32), smoking and alcohol (25,32), and structurally stratified, health behavior, and physical activity (29). In relation to gender and sexual and reproductive health, HL served as a mediator (34) (Table 2).
Table 2.
Studies for a Relationship Between HL and HP of School Adolescents
|
Study Reference
|
Objectives/Hypothesis
|
Variables Used in Relation to HP
|
Results
|
Measures of Associations
|
| Paakkari et al (29) |
To explain health outcomes independently, HL also mediates the association between structural stratification and health outcomes |
Age, gender, school achievement, health behavior, diet, physical activities, sleep duration, perceived health, self-esteem, and education aspiration |
Better health outcomes were linked to higher HL. Indicators of health behaviors and health were all statistically significant predictors of HL similar to all of the background variables. |
Regression model; When non-significant (P > 0.05) paths were omitted, the model fit to the data was excellent [χ2(10) = 15.35, P = 0.12, RMSEA = 0.01, CFI = 1, TLI = 0.99, SRMR = 0.01]. |
| Riiser et al (30) |
To examine the relationship between HL and knowledge and behavior in order to stop the spread of COVID-19. |
HL, health-protective behavior, and HR-QOL |
HL and hand-washing knowledge (0.14; 95% CI [.15:.21]), hand-washing behavior (0.18; 95% CI [.15:.21]), and HR-QOL (b = 0.80; 95% CI [.61:1.0]) are significantly associated. |
Kruskal-Wallis test with post hoc Mann-Whitney U tests; Chi-square test and multiple linear/logistic regression |
| Paakkari et al (31) |
To compare HL among adolescents who participated or did not participate in a sports club. |
HL, member sports club, physical activity, and family affluence. |
Perceived HL was higher among adolescents who participated in sports club activities (P < 0.001). |
Multilevel mixed-effects logistic regression analyses |
| Intarakamhang and Intarakamhang (41) |
To develop a path model of HL for obesity preventive behaviors |
HL and obesity preventive behaviors, (eating, exercise, and emotional coping) |
HL affects the development of obesity prevention behaviors in three different paths. Path 1: Health knowledge and understanding directly influenced eating behavior (effect sized - β was 0.13, P < 0.05); Path 2: Managing their health conditions, media literacy, and appropriate health-related decision making (β = 0.07, 0.98, and 0.05); Path 3: Communicating for added skills, media literacy, and appropriate health-related decision making (β = 0.63, 0.93, 0.98, and 0.05); Path 4: HB through an interactive, and critical level (β = 0.76, 0.97, and 0.55) |
Path analysis model, structure equation model, and causal relationship model |
| Brandt et al (25) |
To examine different components of HL and associations with smoking and alcohol |
HL, smoking, and alcohol |
The lower HL, the more frequently they smoked (b ¼ 0.12, P < .001), and in the last 30 days (b ¼ 0.15, P < .001), alcohol consumption (lifetime: b ¼ 0.03, P < .05; last 30 days: b ¼ 0.07, P < .001) and its beverages on occasions. |
Structural equation models and confirmatory factor analysis |
| Ran et al (26) |
To explore the relationship between QOL and different levels of HL |
HL, QOL, psychological wellbeing, and mental well-being |
Students who were equipped with higher HL had greater QOL (P < 0.01), and this discrimination remained significant in subscales such as physiological well-being (P < 0.01), mental well-being (P < 0.01), social well-being (P < 0.01), and pubertal well-being (P < 0.01). |
Chi-squared tests, t-tests, or F tests were employed to examine the unadjusted associations and regression analysis |
| Valerio et al (27) |
To investigate the relationships between HL and self-care for asthma. |
HL, asthma self-care, and self-efficacy |
REALM-Teen scores were strongly correlated with asthma knowledge and self-efficacy. |
Bivariate associations of each predictor to the REALM-Teen through mixed-effect regression models. |
| Sukys et al (32) |
To examine the relationship between HL, school achievement, health education in schools, and family economic status. |
HL, school achievement,health education (HE) in school, and family affluence |
A significant predictor of HL was school achievement (Pearson’s r = 0.26). Family affluence (r = 0.12) also indicated a higher level of HL. |
Descriptive, ANOVA, post hoc Tukey’s test, Chi-square tests, Pearson’s correlation coefficients, and multiple regression |
| Valerio et al (42) |
To examine the association between HL, asthma management, and QOL |
HL, asthma management, and QOL |
A significant association between inadequate HL and suboptimal asthma management. |
Descriptive statistic: Frequencies, means, SDs, and logistic regression |
| Paakkari et al (34) |
Does HL mediate the association between gender/family affluence and self-rated health? |
HL, gender, self-rated health, and family affluence |
HL is a mediator between gender, family affluence (0.8-2.6% variance), and self-reported health (1.4-7.3%). A significant (P < 0.001) positive association was found between HL and self-reported health in each country. |
Descriptive, ANOVA, univariate ANOVA, and path modeling |
| Ozturk and Ayaz-Alkaya (35) |
Is there any relationship between HL and HP behaviors of adolescents? |
HL, nutrition, interpersonal support, health responsibility, self-realization, exercise, and stress management |
A moderate positive correlation was found between the school-age HL scale and the adolescent HP scale ((r = 0.488, P < 0.001), stress management, (r = 0.412, P < 0.001), and health responsibility (r = 0.444, P < 0.001), as well as a weak positive relationship between HL and nutrition (r = 0.282, P < 0.001), exercise (r = 0.247, P < 0.001), social support (r = 0.365, P < 0.001), and life satisfaction (r = 0.394, P < 0.001). |
Descriptive, ANOVA, Spearman’s correlation coefficient, and a two-sided P-value |
| Zhang et al (39) |
To examine associations between psychosomatic symptoms and HL in junior and senior high school students |
HL and physical and psychological symptoms |
A strongly poor correlation with both psychological symptoms and physical problems (P > 0.05 for each). |
Multiple linear regression,
Mann-Whitney test, Kruskal-Wallis H test, independent-Samples t-test, and one-way ANOVA |
| Yang et al (40) |
Effects of HL on the subgroups of health risk behaviors of adolescent |
HL and health risk behavior low-risk class; Smoking, alcohol, screen time, moderate risks = Non-suicidal self-injury, suicidal behavior, unintentional injury. High-risk = Smoking, alcohol, screening time, non-suicidal self-injury/ behavior, and unintentional injury |
One score of improvement in HL, as compared with the low-risk class, was significantly associated with a 1.0% lower risk among adolescents belonging to the low-risk class and a 3.5% lower relative risk among those with high risk. There was heterogeneity in the profiles of the high-risk classand HL in different classes. |
Mean ± SD, normality test, population rate, confidence interval, and regression mixture modeling |
| Jabeen et al (37) |
Association between HL and health-seeking behavior of adolescents. |
HL and health-seeking behavior |
AHL was minimal and not associated with health-seeking behavior (0.92 |
Spearman rank, correlation coefficient, and the Pearson Chi-square |
| Motamedi et al (38) |
Relationship of BMI with HL and regular physical activity self-efficacy in adolescents aged 15-18. |
HL, BMI, regular physical exercise, and self-efficacy |
A significant difference between the mean scores of students’ HL in the four levels of BMI (P < 0.0001), while no significant relationship between HL and regular physical activity self-efficacy (P = 0.67). |
Mean ± SD, Z test, and P-value |
Note. AHL: Adolescent health literacy; HP: Health promotion; BMI: Body mass index; SD: Standard deviation; ANOVA: Analysis of variance; QOL: Quality of life; COVID-19: Coronavirus disease 19; CI: Confidence interval; RMSEA: Root mean square error of approximation; CFI: Comparative fit index; TLI: Tucker–Lewis index; SRMR: Root mean square residual.
Three studies evaluated the significant relationship between health-related quality of life with HL (26,30,42). Likewise, three studies examined the significant relationship of family influence (31,32,34), physiological and mental well-being (26,39), self-care and asthma (27,42), and self-efficacy (38,42) with HL. One paper reported a significant association between HL and the management of a health condition, appropriate health decision-making, physiological, mental, and social well-being (26,39), street management, and health responsibility (35). Two studies showed that school achievement and availability of health provisions in school were significant predictors of HL (29,32).
Conversely, five articles found no association between HL and HP aspects (35,37-40). One study represented a weak relationship between HL and nutrition, exercise, social support, and life satisfaction (35). As per another study, HL was negatively associated with physical and psychological symptoms (39). Negative correlations were also observed between HL and health risk behavior (40), and health-seeking behavior (37), as well as daily physical exercise, self-efficacy, and four levels of the body mass index (38).
Discussion
This systematic review investigated HL status and how it is measured in the current studies of adolescent HL. The results will also be utilized to determine which scales are currently in use, as well as how they were developed, validated, tested, and employed in this regard (16). Second, the study sought to understand the relationship between adolescent HP and HL levels. According to the number of papers published worldwide during the given time period, the study of adolescent HL is progressing at an encouraging rate.
The review identified 13 HL measures that were used to assess the HL of adolescents in various settings. This inductive work in the field of HL demonstrates that there has been a noteworthy increase in the number of different HL measures for adolescents in the recent academic literature. It was found that most (n = 8) studies employed subjective HL measures, and the HLSAC was the most common one. Additionally, this study reported only five focused FHL instruments, and NVS was the most commonly used one. Many papers apply these two instruments because they are short and accessible. This result does not correspond with earlier findings (16,21,22). In the current review, as compared to earlier studies, the use of multidimensional tools appears to have intensified somewhat from a multidimensional perspective of adolescent HL tools. However, they only reperesented five of the 13 instruments. This review revealed the narrow focus of AHL measures as a solid research inconsistency similar to other studies, implying that the context should not be overlooked when establishing a tool based on a broad theoretical foundation of HL. Thus, the design of multidimeniosal and context-specific tools becomes desirable.
This paper identified fewer HL scales than three other papers (16,21,22) exploring similar issues and more than one other previously conducted review paper (47). These discrepancies could be due tofewer database searches being included in the review and the timing of the review. In addition, only generic HL measures were included. Similarly, the other studies also included children in the sample. Most instruments used a broad and multifaceted notion of HL. It is noted that the number of AHL tools seems to have increased over time. This current review shows that the paradigm of HL measurement is now shifting from objective to subjective. This review identified a total of five new HL tools. Although all the identified scales were constructed in the context of schools, they did not conform to the school context and HP principle. The measures of HL exist for adolescents, but they are not generally accepted across settings. This may have posed a problem for this area of study. Therefore, more research is needed to involve schools’ context, HP principles, and social determinants.
For adolescents, eight self-reported measures of HL were identified in this review. Likewise, few studies utilized tools mainly developed and validated for measuring the HL of adult people. This situation raises the question of whether an adult-specific questionnaire based on a subjective or objective approach can be effectively adopted to measure AHL. Moreover, most studies employed tools developed by others. Can scale made in one country or place be valid in another? Therefore, the HL measure is especially significant when analyzed in a practice-to-practice situation. In the context of this review, there is a great deal of confusion about which of the 13 tools used in the various studies would be viable. Hence, there is a need to build context-based HL scales based on both subjective and objective perspectives. The findings of this study provided basic information on how to develop, test, use, and measure the reliability of HL tools. However, the full details of many of the applied tools have not been stated. The characteristics of the existing scales (e.g., their item number, eligibility requirements, scoring methods, and administration) contain several contradictions and discrepancies. Thus, making the best tool selections is difficult. However, the results of this study will be taken into account to include more details for anyone who wishes to learn more about HL. There is a need to develop and validate a comprehensive or collective HL scale for adolescents contextually using HP perspectives.
Based on the findings of this review, most studies (n = 19) had a cross-sectional design that only provides baseline data. Most studies reported the internal consistency of the applied instruments. Seven studies did not have well-described psychometric properties or failed to mention them. Only one study mentioned the validity of the instrument. HL scales focused on the quantitative validity and reliability of measures for functional, communicative, and critical HL. Due to the lack of methodological aspects and the quality of the research reports, most information on HL scale features remained unclear (21). There was a lack of qualitative measures of critical and interactive HL (4). Mixed-method and interventional study designs are also necessary.
In general, eight studies reported that the HL level of school adolescents was limited in certain countries. The same finding was also provided, indicating the high prevalence of limited HL among adolescents and youths (46,48). There is no evidence of AHL in many countries. Eight studies reported that there are statistically significant correlations with personal factors. The relationship between age, gender, and HL was inconsistent across studies (47), while another review’s finding concurred with this (46).
To conclude this review, 15 studies comprised the relationship of HL with 22 components of HP. Overall, 13 articles examined the relationship of HL with different dimensions of health behaviors of school adolescents. Of these, eight cases showed that health behavior was statistically significantly associated with HL. HL is an independent and positive factor as a mediator for health-promoting behavior. The other reviewed papers demonstrated that there is a meaningful relationship between HL and adolescents’ health behaviors (47), and poorer HL was associated with some adverse health outcomes (46). The findings of this review also represented that studies included only limited aspects of HP. No research was identified on the relationship between HL and HP in adolescents, highlighting the need for examining the relationship between HL and HP among adolescents.
Limitations and Strengths
The first limitation of this review was the omission of any examination of the conceptual perspective of HL. Second, only English-language HL papers were examined in this review. Furthermore, we did not conduct a quality assessment screening of the addressed studies. It was difficult to compare the findings because the age ranges, maturation, cognition, abilities, attitude, self-efficacy, educational level, decision-making, autonomy, and experiences varied between investigations. A further limitation of this study’s search strategy was that it was only applied for five years. Only three reviewable datasets were employed in this investigation. However, to the best of our knowledge, this is the first study to identify the measurement techniques applied in AHL studies, which is considered a strong point. It also established the connection between HP and AHL.
Recommendations
In this study, HP principles were proposed as a basis for developing relevant and contextual measures to assess the level of HL among adolescents. The low level of HL among adolescents calls for the development and implementation of HL programs for them as suggested by Manganello (49). Despite its importance in improving people’s health, HL lacks significant research, which highlights the need to incorporate and study the topic in the near future. Furthermore, compared to cross-sectional studies, experimental and qualitative studies are more limited, suggesting the need for such studies.
Conclusion
In the review, it was suggested that AHL measurement tools are becoming increasingly popular with different types of measurements, although the characteristics of the tools differ widely. As a result, researchers interested in this field face both opportunities and challenges. In addition, the evaluation of contemporary papers demonstrates evidence that children have a low HL. The findings of the current review study highlighted the need for interventional and action research for AHL promotion. It was concluded that the HL of school adolescents is statistically significant for their HP. It is an independent factor and a positive mediator in numerous areas of HP. The results of this review revealed that there is a scarcity of HL and HP research among school adolescents, emphasizing the need to conduct action and interventional research on the relationship between literacy and HP in the future, including multi-levels and multi-factors of HL.
Authors’ Contribution
Conceptualization: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Orkan Okan, Edwin van Teijlingen, Mohan Kumar Sharma, Jib Acharya, Cate Wood.
Data curation: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Orkan Okan.
Formal analysis: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Mohan Kumar Sharma.
Funding acquisition: No funding support
Investigation: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Orkan Okan, Edwin van Teijlingen.
Methodology: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Orkan Okan, Edwin van Teijlingen.
Project administration: Shanti Prasad Khanal.
Resources: Shanti Prasad Khanal, Orkan Okan, Edwin van Teijlingen, Jib Acharya.
Software: Shanti Prasad Khanal.
Supervision: Chitra Bahadur Budhathoki, Orkan Okan.
Validation: Orkan Okan, Edwin van Teijlingen.
Visualization: Chitra Bahadur Budhathoki, Cate Wood.
Writing – original draft: Shanti Prasad Khanal, Chitra Bahadur Budhathoki, Orkan Okan, Edwin van Teijlingen, Mohan Kumar sharma
Writing – review & editing: Shanti Prasad, Orkan Okan, Edwin van Teijlingen, Jib Acharya, Cate Wood.
Competing Interests
Authors declare that they have no conflict of interests.
Ethical Approval
Not applicable.
Supplementary Files
Supplementary file 1 contains Table S1.
(pdf)
References
- Simonds SK. Health education as social policy. Health Educ Monogr 1974; 2(1 Suppl):1-10. doi: 10.1177/10901981740020s102 [Crossref] [ Google Scholar]
- Institute of Medicine. In: Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- World Health Organization. Health Literacy Toolkit for Low- And Middle-Income Countries: A Series of Information Sheets to Empower Communities and Strengthen Health Systems. New Delhi: WHO Regional Office for South-East Asia; 2015.
- Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int 2000; 15(3):259-67. doi: 10.1093/heapro/15.3.259 [Crossref] [ Google Scholar]
- Vamos S, Okan O, Sentell T, Rootman I. Making a case for “Education for health literacy”: an international perspective. Int J Environ Res Public Health 2020; 17(4):1436. doi: 10.3390/ijerph17041436 [Crossref] [ Google Scholar]
- Paakkari L, Paakkari O. Health literacy as a learning outcome in schools. Health Educ 2012; 112(2):133-52. doi: 10.1108/09654281211203411 [Crossref] [ Google Scholar]
- Okan O. From Saranac Lake to Shanghai: a brief history of health literacy. In: Okan O, Bauer U, Levin-Zamir D, Pinheiro P, Sørensen K, eds. International Handbook Health Literacy: Research, Practice and Policy Across the Lifespan. Bristol, UK: Policy Press; 2019. p. 21-38.
- Nutbeam D. Discussion Paper on Promoting, Measuring and Implementing Health Literacy-Implications for Policy and Practice in Non-Communicable Disease Prevention and Control. World Health Organization; 2017. p. 1-29.
- Ratzan SC, Parker RM, Selden C, Zorn M. National Library of Medicine Current Bibliographies in Medicine: Health Literacy. Bethesda, MD: National Institutes of Health; 2000.
- Barzanjeh Atri S, Sahebihagh MH, Asghari Jafarabadi M, Behshid M, Ghasempour M, Abri F. The relationship between health literacy and stages of change in smoking behavior among employees of educational health centers of Tabriz University of Medical Sciences (2016). Int J Prev Med 2018; 9:91. doi: 10.4103/ijpvm.IJPVM_259_17 [Crossref] [ Google Scholar]
- Shum J, Poureslami I, Doyle-Waters MM, FitzGerald JM. The application of health literacy measurement tools (collective or individual domains) in assessing chronic disease management: a systematic review protocol. Syst Rev 2016; 5:97. doi: 10.1186/s13643-016-0267-8 [Crossref] [ Google Scholar]
- Kanj M, Mitic W. Health literacy and health promotion: definitions, concepts and examples in the Eastern Mediterranean region. In: 7th Global Conference on Health Promotion Promoting Health and Development: Closing the Implementation Gap. Geneva: World Health Organization; 2009.
- Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health 2012; 12:80. doi: 10.1186/1471-2458-12-80 [Crossref] [ Google Scholar]
- Abacigil F, Harlak H, Okyay P, Kiraz DE, Gursoy Turan S, Saruhan G. Validity and reliability of the Turkish version of the European Health Literacy Survey Questionnaire. Health Promot Int 2019; 34(4):658-67. doi: 10.1093/heapro/day020 [Crossref] [ Google Scholar]
- Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM. Health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health 2017; 17(1):361. doi: 10.1186/s12889-017-4267-y [Crossref] [ Google Scholar]
- Okan O, Lopes E, Bollweg TM, Bröder J, Messer M, Bruland D. Generic health literacy measurement instruments for children and adolescents: a systematic review of the literature. BMC Public Health 2018; 18(1):166. doi: 10.1186/s12889-018-5054-0 [Crossref] [ Google Scholar]
- Mansfield R, Patalay P, Humphrey N. A systematic literature review of existing conceptualisation and measurement of mental health literacy in adolescent research: current challenges and inconsistencies. BMC Public Health 2020;20(1):607. Published 2020 May 1. 10.1186/s12889-020-08734-1.
- Massey PM, Prelip M, Calimlim BM, Quiter ES, Glik DC. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Health Educ Res 2012; 27(6):961-74. doi: 10.1093/her/cys054 [Crossref] [ Google Scholar]
- Altin SV, Finke I, Kautz-Freimuth S, Stock S. The evolution of health literacy assessment tools: a systematic review. BMC Public Health 2014; 14:1207. doi: 10.1186/1471-2458-14-1207 [Crossref] [ Google Scholar]
- Nutbeam D. Defining, measuring and improving health literacy. Health Evaluation and Promotion 2015; 42(4):450-5. doi: 10.7143/jhep.42.450 [Crossref] [ Google Scholar]
- Guo S, Armstrong R, Waters E, Sathish T, Alif SM, Browne GR. Quality of health literacy instruments used in children and adolescents: a systematic review. BMJ Open 2018; 8(6):e020080. doi: 10.1136/bmjopen-2017-020080 [Crossref] [ Google Scholar]
- Ormshaw MJ, Paakkari LT, Kannas LK. Measuring child and adolescent health literacy: a systematic review of literature. Health Educ 2013; 113(5):433-55. doi: 10.1108/he-07-2012-0039 [Crossref] [ Google Scholar]
- Selçuk AA. A guide for systematic reviews: PRISMA. Turk Arch Otorhinolaryngol 2019; 57(1):57-8. doi: 10.5152/tao.2019.4058 [Crossref] [ Google Scholar]
- Pathak RS, Teijlingen Ev, Padam Simkhada, Bhimsen Devkota, Poobalan A, Regmi P, et al. Workshop handbook: Systematic review: Partnership on improving Access to Research Literature for Higher Education Institutions in Nepal (PARI); 2012.
- Brandt L, Schultes MT, Yanagida T, Maier G, Kollmayer M, Spiel C. Differential associations of health literacy with Austrian adolescents’ tobacco and alcohol use. Public Health 2019; 174:74-82. doi: 10.1016/j.puhe.2019.05.033 [Crossref] [ Google Scholar]
- Ran M, Peng L, Liu Q, Pender M, He F, Wang H. The association between quality of life(QOL) and health literacy among junior middle school students: a cross-sectional study. BMC Public Health 2018; 18(1):1183. doi: 10.1186/s12889-018-6082-5 [Crossref] [ Google Scholar]
- Valerio MA, George M, Liu J, Osakwe ZT, Bruzzese JM. Health literacy and asthma among Hispanic and African-American urban adolescents with undiagnosed asthma. Ann Allergy Asthma Immunol 2018; 121(4):499-500. doi: 10.1016/j.anai.2018.06.022 [Crossref] [ Google Scholar]
- Ghanbari S, Ramezankhani A, Montazeri A, Mehrabi Y. Health literacy measure for adolescents (HELMA): development and psychometric properties. PLoS One 2016; 11(2):e0149202. doi: 10.1371/journal.pone.0149202 [Crossref] [ Google Scholar]
- Paakkari LT, Torppa MP, Paakkari OP, Välimaa RS, Ojala KSA, Tynjälä JA. Does health literacy explain the link between structural stratifiers and adolescent health?. Eur J Public Health 2019; 29(5):919-24. doi: 10.1093/eurpub/ckz011 [Crossref] [ Google Scholar]
- Riiser K, Helseth S, Haraldstad K, Torbjørnsen A, Richardsen KR. Adolescents’ health literacy, health protective measures, and health-related quality of life during the COVID-19 pandemic. PLoS One 2020; 15(8):e0238161. doi: 10.1371/journal.pone.0238161 [Crossref] [ Google Scholar]
- Paakkari L, Kokko S, Villberg J, Paakkari O, Tynjälä J. Health literacy and participation in sports club activities among adolescents. Scand J Public Health 2017; 45(8):854-60. doi: 10.1177/1403494817714189 [Crossref] [ Google Scholar]
- Sukys S, Trinkuniene L, Tilindiene I. Subjective health literacy among school-aged children: first evidence from Lithuania. Int J Environ Res Public Health 2019; 16(18):3397. doi: 10.3390/ijerph16183397 [Crossref] [ Google Scholar]
- Paakkari O, Torppa M, Boberova Z, Välimaa R, Maier G, Mazur J. The cross-national measurement invariance of the health literacy for school-aged children (HLSAC) instrument. Eur J Public Health 2019; 29(3):432-6. doi: 10.1093/eurpub/cky229 [Crossref] [ Google Scholar]
- Paakkari L, Torppa M, Mazur J, Boberova Z, Sudeck G, Kalman M. A comparative study on adolescents’ health literacy in Europe: findings from the HBSC Study. Int J Environ Res Public Health 2020; 17(10):3543. doi: 10.3390/ijerph17103543 [Crossref] [ Google Scholar]
- Ozturk FO, Ayaz-Alkaya S. Health literacy and health promotion behaviors of adolescents in Turkey. J Pediatr Nurs 2020; 54:e31-e5. doi: 10.1016/j.pedn.2020.04.019 [Crossref] [ Google Scholar]
- Caldwell EP, Melton K. Health literacy of adolescents. J Pediatr Nurs 2020; 55:116-9. doi: 10.1016/j.pedn.2020.08.020 [Crossref] [ Google Scholar]
- Jabeen R, Rehman MU, Masood S, Mahmood H, Mashhadi SF. Assessment of functional health literacy among adolescents of model schools of Islamabad. Pak Armed Forces Med J 2018; 68(3):545-9. [ Google Scholar]
- Motamedi M, Peyman N, Afzalaghaee M. Rrelationship of health literacy and regular physical activity self-efficacy with body mass index in adolescent girls aged 15-18 years. J Health Lit 2020; 5(3):64-73. doi: 10.22038/jhl.2020.51448.1123 [Crossref] [ Google Scholar]
- Zhang SC, Li DL, Yang R, Wan YH, Tao FB, Fang J. The association between health literacy and psychosomatic symptoms of adolescents in China: a cross-sectional study. BMC Public Health 2019; 19(1):1259. doi: 10.1186/s12889-019-7589-0 [Crossref] [ Google Scholar]
- Yang R, Li D, Hu J, Tian R, Wan Y, Tao F. Association between health literacy and subgroups of health risk behaviors among Chinese adolescents in six cities: a study using regression mixture modeling. Int J Environ Res Public Health 2019; 16(19):3680. doi: 10.3390/ijerph16193680 [Crossref] [ Google Scholar]
- Intarakamhang U, Intarakamhang P. Health literacy scale and causal model of childhood overweight. J Res Health Sci 2017; 17(1):e00368. [ Google Scholar]
- Valerio MA, Peterson EL, Wittich AR, Joseph CL. Examining health literacy among urban African-American adolescents with asthma. J Asthma 2016; 53(10):1041-7. doi: 10.1080/02770903.2016.1175473 [Crossref] [ Google Scholar]
- Hughes D, Maiden K. Navigating the health care system: an adolescent health literacy unit for high schools. J Sch Health 2018; 88(5):341-9. doi: 10.1111/josh.12616 [Crossref] [ Google Scholar]
- Sarhan MBA, Shannon HS, Fujiya R, Jimba M, Giacaman R. Psychometric properties of an Arabic-language health literacy assessment scale for adolescents (HAS-A-AR) in Palestine. BMJ Open 2020; 10(6):e034943. doi: 10.1136/bmjopen-2019-034943 [Crossref] [ Google Scholar]
- Tsubakita T, Kawazoe N, Ichikawa M, Matsumoto S, Sugawara M. Assessing knowledge-based and perceived health literacy among Japanese adolescents: a cross-sectional study. Glob Pediatr Health 2020; 7:2333794x20944311. doi: 10.1177/2333794x20944311 [Crossref] [ Google Scholar]
- Sansom-Daly UM, Lin M, Robertson EG, Wakefield CE, McGill BC, Girgis A. Health literacy in adolescents and young adults: an updated review. J Adolesc Young Adult Oncol 2016; 5(2):106-18. doi: 10.1089/jayao.2015.0059 [Crossref] [ Google Scholar]
- Fleary SA, Joseph P, Pappagianopoulos JE. Adolescent health literacy and health behaviors: a systematic review. J Adolesc 2018; 62:116-27. doi: 10.1016/j.adolescence.2017.11.010 [Crossref] [ Google Scholar]
- Khanal SP, Budhathoki CB, Okan O. Improving adolescent health literacy through school-based health literacy intervention: a mixed-method study protocol. BMC Public Health 2023;23(1):407. Published 2023 Feb 28. 10.1186/s12889-023-15316-407.
- Manganello JA. Health literacy and adolescents: a framework and agenda for future research. Health Educ Res 2008; 23(5):840-7. doi: 10.1093/her/cym069 [Crossref] [ Google Scholar]