J Educ Community Health. 11(4):222-229.
doi: 10.34172/jech.3326
Original Article
A Comprehensive Health Assessment of the Khezr Neighborhood in Hamedan, Iran: Identifying Key Issues for 2024
Sanaz Omidi 1  , Mansour Salehpour 1, Reza Bigdeli 1, Zahra Yazdanian 1, Parham Mohammadi 1, Mehdi Mousavi 1, Saber Ghaffari 1, Abouzar Raeisvandi 1, Younes Mohammadi 1, 2, *
, Mansour Salehpour 1, Reza Bigdeli 1, Zahra Yazdanian 1, Parham Mohammadi 1, Mehdi Mousavi 1, Saber Ghaffari 1, Abouzar Raeisvandi 1, Younes Mohammadi 1, 2, *
Author information:
1Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
2Social Determinants of Health Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: Promoting community health is a key priority for enhancing societal well-being. Every health system has the responsibility to address the health challenges faced by communities and must engage in proper planning to resolve priority issues within the scope of available resources. This cross-sectional study was conducted in the Khezr region of Hamadan in 2024, aiming at identifying and prioritizing the problems and needs of the region through direct community participation using the North Carolina model.
Methods: To this end, the region’s issues were identified through focus group discussions, interviews with residents, questionnaires, consultations with local experts, and discussions with some local officials. The criteria for prioritizing these issues included the severity of the problem, its potential consequences, the feasibility of resolution, and the urgency of addressing the issue.
Results: This study enrolled 124 participants, with a mean age of 40.22 years. The Khezr region faced challenges in health services (30.6% dissatisfaction), safety (43.5% unsafe), and economic conditions (84.7% low-income impact). Major health issues included diabetes (89.5%) and high cholesterol (83.1%). Moreover, notable social concerns were poverty, unemployment, and addiction, highlighting the need for targeted interventions.
Conclusion: The problems identified and prioritized in this study span across cultural, social, and economic dimensions, not just health-related concerns. Poverty and unemployment were highlighted as critical issues with significant consequences, requiring both the support of local authorities and the active engagement of the community for effective resolution.
Keywords: Community health assessment, Health prioritization, North Carolina model, Iran
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Omidi S, Salehpour M, Bigdeli R, Yazdanian Z, Mohammadi P, Mousavi M, et al. A comprehensive health assessment of the Khezr neighborhood in Hamedan, Iran: identifying key issues for 2024. J Educ Community Health. 2024; 11(4):222-229. doi:10.34172/jech.3326
Introduction
Community health assessment systematically evaluates a community’s health status, needs, and resources (1), helping in identifying and prioritizing health problems essential for effective service delivery. Progress hinges on a deep understanding of these issues, with successful interventions requiring active community involvement (2). A multidimensional approach, integrating political, social, and biological factors, is vital to addressing societal challenges (3). Globally, health systems collect and analyze data to improve community life quality (4).
These assessments assist policymakers by highlighting strengths and weaknesses and guiding program design to improve public health. The process actively involves community members, from collecting data to identifying issues and proposing solutions (5,6). Community participation ensures they directly contribute to the evaluation (7). The primary goal is to enhance public health through objectives such as having access to better healthcare, reducing preventive care barriers, and encouraging healthier lifestyles (8). The first and most important step in achieving these goals is a complete understanding of the community and awareness of the habits and behaviors of the people living there (9). Understanding community behaviors is key to identifying needs, though incomplete or unreliable data often result in ineffective policies (10).
One effective framework for this process is the North Carolina model, providing tools for data collection, interpretation, and prioritization of health issues. This model prevents redundancy and increases community engagement (2,8). Numerous studies have used similar methods to address societal problems through community cooperation (7,8,11-14). For instance, research in Bandar Abbas and Tehran identified critical issues such as unemployment, poverty, and infrastructure problems (11,12).
In 2023, a study in Chelicheh county identified issues such as drinking water pollution and economic challenges (15), while a 2022 study in Sufian highlighted problems such as early marriage and industrial pollution (14). These assessments help health networks design targeted service programs, fostering collaboration between organizations and community members. This study uses the North Carolina model to identify and prioritize local health problems with direct resident involvement.
Materials and Methods
This cross-sectional study was performed in the Khezr region of Hamadan, Hamedan province, Iran, in 2024. The study was based on the MSc Community Health Assessment Course model from the School of Public Health at Hamadan University of Medical Sciences and the North Carolina Community Assessment Model, a well-established and advanced methodology used internationally.
The rationale for selecting the North Carolina model for this study is explained as follows:
-
Participatory and community-centered framework: The North Carolina model prioritizes active community engagement in identifying health issues and determining priorities. In addition, this participatory approach ensures that the findings are grounded in the lived experiences of the community, making the results more relevant and reflective of local needs. This is particularly critical in settings where a deep understanding of local dynamics is essential for addressing health challenges effectively.
-
Emphasis on evidence-based decision-making: A key strength of the North Carolina model is its reliance on empirical data and evidence to guide decision-making processes. Given the primary objective of this study—to identify and prioritize health needs—this model facilitates an evidence-driven approach, ensuring that decisions are rooted in reliable data, thereby enhancing their validity and effectiveness.
-
Alignment with local resources and context: The model’s focus on leveraging local resources and assets ensures that interventions are contextually appropriate and sustainable. In regions with constrained resources, this approach maximizes the potential impact of health interventions by utilizing existing local capacities, which contributes to the long-term success and sustainability of the initiatives.
-
Flexibility in tailoring health interventions: One of the distinctive features of the North Carolina model is its adaptability, which allows for the customization of health interventions to fit the unique needs and conditions of specific regions. This flexibility is particularly valuable in addressing the diverse and evolving health challenges that may arise within a community, ensuring that interventions remain relevant and responsive to local circumstances.
The North Carolina model operates in two phases. Phase 1 (stages 1–7) focuses on identifying problems, while phase 2 is dedicated to developing action plans to address those problems. This paper presents the results of the first phase of the study.
Stage 1: Formation of the Assessment Team
In this stage, a community health assessment team was formed, comprising a working group, a consultant group, and a project supervisor. The working group consisted of five master’s students and three Ph.D. students in epidemiology. The project supervisor, a faculty member from Hamadan University of Medical Sciences, supervised the entire process, including coordinating the program, ensuring accuracy, and responding to authorities and partner organizations.
Stage 2: Primary Data Collection
The focus of this stage was the collection of primary data. The Community Health Assessment Team collected data through questionnaires, gathering the views and concerns of local residents about various aspects of life, including health. The data were vital for assessing the community’s status from the residents’ perspective. Qualitative data were gathered via interviews and focus group discussions with key community members, such as local officials and staff from the Khezr Health Center. These discussions highlighted the region’s strengths and weaknesses. Additionally, interviews were conducted with 124 residents using an available sampling method in public areas, such as parks and bazaars. The interviews were conducted face-to-face using open-ended questions, and each participant’s views on the region’s key health issues were recorded by the researchers.
The questionnaire comprised seven sections related to demographic information, quality of life, community development (e.g., literacy and health awareness), health information, personal health, access to family care and health services, and emergency preparedness.
Moreover, this questionnaire, modeled after the standard questionnaire in the Community Health Assessment textbook (16), consisted of 30 questions. Some of them were modified or removed to better suit local culture, while questions on health conditions, such as hypertension, diabetes, cancer, and lifestyle factors, were added. Respondents were asked to rate the importance of identified problems and needs on a scale from 0 (least important) to 10 (most important). During the interviews and discussions, a team member took notes, summarizing participants’ statements to ensure accurate understanding. This process allowed the team to gather a wide range of concerns and suggestions from the community.
Stage 3: Secondary Data Collection and Analysis
This stage involved gathering and analyzing secondary data from sources such as the Hamadan Provincial Health Center and the Hamedan Khezr Comprehensive Health Services Center. The team compared health statistics from the Khezr region with provincial statistics to identify and prioritize community health problems. Data were obtained from the integrated health system, which included health indicators, such as mortality rates, population demographics, disease prevalence, fertility rates, and marriage and divorce statistics. This comparison enabled the team to integrate the views of the community with official health data, leading to a comprehensive understanding of the region’s key health challenges.
Stage 4: Integration of Primary and Secondary Data
In this stage, the primary data collected in stage 2 were combined with the secondary data from stage 3. By comparing these two sources, the team gained a deeper understanding of the major health issues in the Khezr region. This integration of data provided a more complete picture of the region’s needs and challenges, laying the foundation for future planning in community health improvement.
Stage 5: Prioritization of Health Problems
The results of the assessment were presented to local health authorities in the Khezr region, with a prioritized list of health issues. Using the Hanlon matrix, the identified problems were ranked based on criteria such as the magnitude of the problem, its seriousness, the ease of solving it, and its urgency. Forms were distributed among the working group members to evaluate these factors for each issue. Each criterion was scored on a scale ranging from 1 (low) to 5 (high). The total possible score for each problem ranged from 4 to 20. By calculating the average score for each issue, the health problems were ranked from highest to lowest priority.
Stages 6 and 7: Documentation and Dissemination
The final stages were dedicated to documenting and publishing the results of the community health assessment. The assessment team compiled a report detailing the evaluation process, the methods used to identify and prioritize problems, and the findings. The goal was to share these results with the community and other stakeholders, fostering collaboration and consensus in future efforts to address the region’s health challenges. With the publication of this report, it is hoped that the community will be better equipped to plan and implement effective solutions to the problems identified.
Results
Following interviews and group discussions with officials and various community members, primary data were collected to examine the challenges faced by the Khezr region. After gathering and analyzing secondary data, the total population of the Khezr region was determined to be 13,287 people and 4525 households, according to the 2024 census. In early 2024, the population < 1 year of age and < 5 years was 176 and 813, respectively. The leading causes of death in the region were cardiovascular diseases (n = 6), cancer (n = 2), suicide (n = 2), traffic accidents (n = 2), and other causes (n = 2). The demographic information of the participants in the study is presented in Table 1. Primary and secondary data from the Khezr Health Center were consolidated, and after eliminating overlapping issues raised in different sessions. The identified issues in the Khezr area of Hamedan from the perspective of the people are provided in Table 2. Additionally, based on the Hanlon Matrix, the 10 key problems of the area, in order of priority, are presented in Table 3 and Figure 1. Table 1 summarizes the demographic characteristics of the participants. A total of 124 participants were enrolled in the study, with a mean age of 40.22 ± 14.95 years. The mean age was 42.89 ± 14.85 years for men and 35 ± 13.88 years for women (P = 0.005). Of the participants, 82 (66.1%) were male, and 42 (33.9%) were female. The majority of participants (72, 58.1%) identified as Turkish. Regarding marital status, 41 (33.1%), 71 (57.3%), 7 (5.6%), and 5 (4%) were single, married, divorced, and widowed, respectively. Most participants had an education level below a diploma, with 54 (43.5%) holding this level of education. Employment data revealed that 43 (34.7%) participants were employed, with a mean age of 40.51 ± 9.86 years and 36.40 ± 16.10 years for the employed and unemployed groups, respectively. The unemployment rate was 47.1%, with 20.4%, 36.3%, and 6.5% unemployment among those with education below high school, high school education, and a university degree, respectively. Unemployment rates were 36.6%, 57.3%, 5.6%, and 4% for single, married, divorced, and widowed individuals, respectively. Gender-wise, the unemployment rate was 16.7% among women and 34.1% among men. Unemployment rates across ethnic groups were 25.9%, 25%, 25%, and 47.1% for Fars, Turkish, Lur, and Kurdish ethnicities, respectively.
Table 1.
Demographic Characteristics and Other Information From the Community Health Assessment Study in the Khezr Region (2024)
|
Variable
|
Mean±SD or No. (%)
|
| Age |
40.22 ± 14.95 |
| Gender |
|
| Female |
42 (33.9) |
| Male |
82 (66.1) |
| Ethnicity |
|
| Persian |
27 (21.8) |
| Turkish |
72 (58.1) |
| Lore |
8 (6.5) |
| Kurdish |
17 (13.7) |
| Marital status |
|
| Single |
41 (33.1) |
| Married |
71 (57.3) |
| Divorced |
7 (5.6) |
| Widow |
5 (4) |
| Education |
|
| Illiterate |
17 (13.7) |
| Below high school |
54 (43.5) |
| High school |
45 (36.6) |
| University |
8 (6.5) |
| Employment status |
|
| Employed |
43 (34.7) |
| Unemployed |
35 (28.2) |
| Retired |
16 (13.7) |
| Homemaker |
24 (19.4) |
| Student |
5 (4) |
Note. SD: Standard deviation.
Table 2.
Community Quality of Life, Economic and Social Conditions, Health Information, Personal Health, Access to Healthcare, and Emergency Preparedness
|
Heading
|
Subheading
|
Details
|
| Community quality of life |
Dissatisfaction with health services |
30.6% of respondents expressed dissatisfaction. |
| Perceived safety |
43.5% felt that the area was not safe. |
| Community cooperation |
42.7% agreed that there was a sense of cooperation and support. |
| Suitability for the elderly |
32.3% disagreed that the region was suitable for elderly residents. |
| Economic and social conditions |
Impact of poverty |
84.7% identified low income and poverty as major factors affecting the quality of life. |
| Employment |
64.5% reported access to employment as a pressing need. |
| Robbery |
54.8% cited robbery as having a significant impact on living conditions. |
| Health information |
Sources of information |
49.24%, 44.4%, and 44.4% received information from friends and family, cyberspace (e.g., Instagram, Telegram, and WhatsApp), and television and radio, respectively. |
| Personal health |
Priority health topics |
Routine check-ups (73.6%), anger management (71.8%), smoking cessation (71%), crime prevention (71%), and substance/alcohol abuse prevention (70.2%). |
| Children’s health needs |
Oral hygiene (45.2%), nutrition (39.5%), mental health (29%), tobacco/hookah smoking (28.2%), and sexually transmitted diseases (22.6%). |
| Health status |
28.2% reported poor health. |
| Common health issues |
Depression/anxiety (21.8%), hypertension (20.2%), high cholesterol (83.1%), diabetes (89.5%), and cardiovascular disease (17.7%). |
| Barriers to physical activity |
Heavy work demands, lack of facilities, and high cost of sports clubs. |
| Access to healthcare |
Healthcare facilities |
Lack of hospitals (33.9%) and private clinics (29.8%). |
| Insurance issues |
Health insurance unavailable (40.3%), insufficient insurance coverage (37.9%), and pharmacies not accepting insurance (56.5%). |
| Pediatric services |
Lack of pediatricians (34.7%). |
| Emergency preparedness |
Preparedness kits |
67% lacked emergency preparedness kits at home. |
| Information sources |
54.7% received information about natural disasters via television. |
Table 3.
Top 10 Problems in Khezr Region Using the Hanlon Matrix
|
Row
|
Problem
|
Magnitude (1-10)
|
Seriousness (1-10)
|
Correctability (1-10)
|
Total
|
| 1 |
Low income/poverty |
9.15 |
9.25 |
4.13 |
22.53 |
| 2 |
Unemployment |
8.14 |
7.44 |
6.38 |
21.96 |
| 3 |
Addiction and drug use |
7.75 |
8.22 |
4.88 |
20.85 |
| 4 |
Depression or anxiety |
8.10 |
7.11 |
5.12 |
20.33 |
| 5 |
School dropouts |
6.13 |
6.01 |
7.63 |
19.77 |
| 6 |
Violent crimes (murder and assault) |
6.75 |
6.25 |
6.48 |
19.48 |
| 7 |
Lack or inadequacy of health insurance |
5.75 |
7.14 |
6.13 |
19.02 |
| 8 |
Theft |
7.88 |
5.50 |
5.38 |
18.76 |
| 9 |
Lack of community support |
8.25 |
5.14 |
5.24 |
18.63 |
| 10 |
Risky driving |
5.77 |
4.29 |
7.38 |
18.44 |
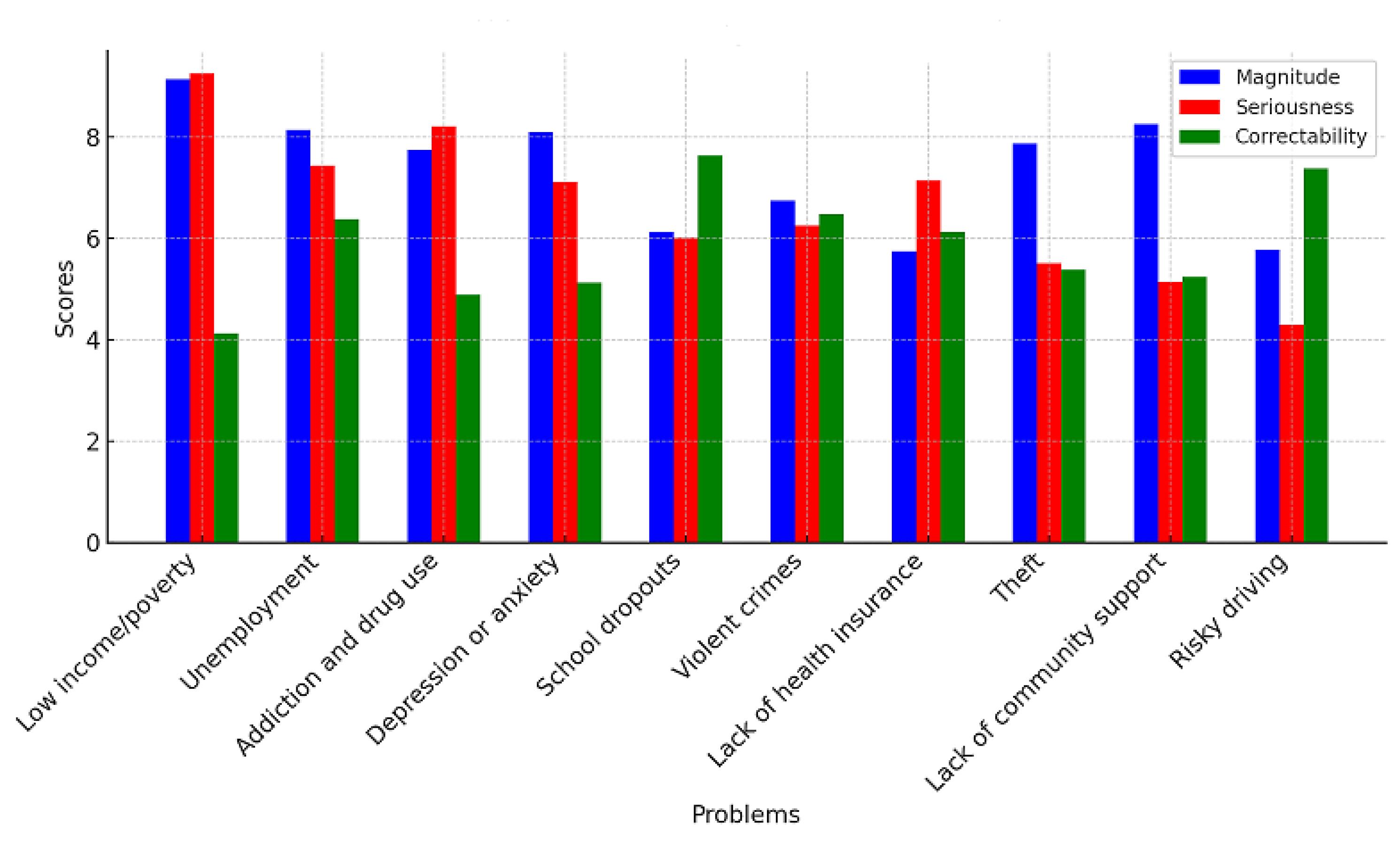
Figure 1.
The Most Important Identified Issues in the Khezr Area of Hamedan Based on the Hanlon Matrix
.
The Most Important Identified Issues in the Khezr Area of Hamedan Based on the Hanlon Matrix
Community Quality of Life
Regarding the quality of life in the Khezr region, 30.6% of respondents expressed dissatisfaction with the provision of health services. Additionally, 43.5% of them felt that the Khezr area was not a safe place to live. However, 42.7% agreed that there was a sense of cooperation and support within the community when people needed help. Meanwhile, 32.3% disagreed that the region was suitable for elderly residents (Table 2).
Economic and Social Conditions
The study results on social progress revealed that 84.7% of respondents believed that low income and poverty had the greatest impact on the quality of life in the Khezr region. Further, access to employment was identified as a pressing need by 64.5% of respondents. Finally, 54.8% cited robbery as having the greatest effect on living conditions in the area (Table 2).
Health Information
Most respondents (49.24%) reported that they received information from friends and family, followed by cyberspace sources, such as Instagram, Telegram, and WhatsApp (44.4%), as well as television and radio (44.4%). The majority of them (73.6%) believed that the residents needed information about routine medical checkups and screenings. Other areas of concern were anger management (71.8%), smoking cessation (71%), crime prevention (71%), substance and alcohol abuse prevention (70.2%), and oral hygiene (65.3%). In addition, respondents indicated that children needed information on oral hygiene (45.2%), nutrition (39.5%), mental health (29%), tobacco and hookah smoking (28.2%), and sexually transmitted diseases, such as AIDS and hepatitis (22.6%). The related data are provided in Table 2.
Personal Health
In the personal health section, 28.2% of respondents reported their health as poor. Common health issues included depression and anxiety (21.8%), hypertension (20.2%), high cholesterol (83.1%), diabetes (89.5%), and cardiovascular disease (17.7%). Many respondents stated they did not engage in physical activities due to heavy work demands, lack of access to suitable exercise facilities, and the high cost of sports clubs (Table 2). The target population of this research may be influenced by specific factors, such as social, economic, and environmental conditions. High levels of stress, lack of access to healthcare services, and sedentary lifestyles can be significant contributors to the increased prevalence of issues, such as diabetes and high cholesterol. Physical inactivity is recognized as an important risk factor in the development of these diseases.
Access to Healthcare
Regarding access to family care and health services, significant issues were identified (Table 2), including the lack of hospitals (33.9%), private clinics (29.8%), health insurance (40.3%), and full insurance coverage (37.9%). Other problems encompassed pharmacies not accepting insurance (56.5%), a lack of pediatricians (34.7%), and insufficient health insurance (33.1%).
Emergency Preparedness
Eventually, 67% of respondents stated they did not have an emergency preparedness kit at home. Most respondents (54.7%) mentioned that they received information about natural disasters through television (Table 2).
Table 3 highlights the top ten problems in the Khezr region, ranked by their overall priority scores, calculated using the Hanlon Matrix. Each problem was assessed based on magnitude, seriousness, and correctability.
Low income and poverty (Total Score: 22.53): Poverty (low income) emerged as the most pressing issue in the region, with high scores for magnitude (9.15) and seriousness (9.25), indicating its widespread impact and critical nature. However, the relatively lower correctability score (4.13) suggests challenges in addressing this issue effectively.
Unemployment (Total Score: 21.96): Unemployment ranked second, with significant scores in all dimensions, particularly correctability (6.38), highlighting both its importance and potential for improvement with targeted interventions.
Addiction and drug use (Total Score: 20.85): This issue demonstrated high seriousness (8.22) and magnitude (7.75), reflecting its detrimental impact on the community. Correctability was moderate (4.88), suggesting some challenges in mitigating this problem.
Depression or anxiety (Total Score: 20.33): Mental health concerns ranked fourth, with high magnitude (8.10) and moderate correctability (5.12), emphasizing the need for accessible mental health services in the region.
School dropouts (Total Score: 19.77): School dropouts, with a correctability score of 7.63, indicated potential for improvement through educational reforms and support programs despite moderate seriousness (6.01).
Violent crimes (murder and assault) (Total Score: 19.48): Violent crimes were rated moderately across all criteria, underlining their disruptive effect on community safety and the importance of law enforcement and preventative measures.
Lack of or inadequacy of health insurance (Total Score: 19.02): Health insurance deficiencies were rated higher in seriousness (7.14) but lower in magnitude (5.75) and correctability (6.13), indicating a complex challenge that affects access to healthcare.
Theft (Total Score: 18.76): It scored higher in magnitude (7.88) but lower in seriousness (5.50), pointing to its impact on daily life without being as critical as other problems.
Lack of community support (Total Score: 18.63): It showed a high magnitude (8.25) but low seriousness (5.14), reflecting its importance in fostering a collaborative and supportive environment.
Risky driving (Total Score: 18.44): Risky driving, though lower in magnitude (5.77) and seriousness (4.29), had a high correctability score (7.38), implying that it is an actionable issue that can be improved with road safety measures.
Discussion
This study identified and prioritized the problems and needs of the Khezr region of Hamadan in 2024 by utilizing the North Carolina method of community evaluation, which integrates both the opinions of the region’s residents and local officials to provide a comprehensive overview of the health and social issues facing this region. By ensuring community participation, it was possible to collect information that more accurately reflected the real needs and challenges of the people in this area.
The results of the study highlighted a variety of problems facing the Khezr region. These problems ranged from economic issues, including low income and poverty, to social concerns, such as unemployment, addiction, drug abuse, school dropouts, depression, anxiety, and violent crimes (including murder and assault). Additional issues encompassed inadequate health insurance, theft, lack of community support, and risky driving behaviors. These identified problems touch on various aspects of individual and communal well-being, ranging from the quality of life to healthcare access, personal health, community development, and emergency preparedness.
Some studies have been conducted both in Iran and globally, exploring community health assessments. For example, Shekari et al assessed the Sufian region, where they identified early marriage among girls, excessive use of chemical fertilizers in agriculture, lack of social security clinics, severe atmospheric pollution caused by industrial waste burning, and insufficient infrastructure in the Mehr Housing area, among other concerns. Their findings revealed a wide array of social, cultural, economic, and health-related problems (14). Similarly, Keykavoos Iranag et al performed a study in Basmanj (Tabriz), identifying youth addiction, urban waste issues, stray dogs, environmental pollution from the Pars Chlorine factory, narrow streets, livestock farms within urban areas, early marriage of girls, urban sewage problems, youth unemployment, and overuse of antibiotics (17). The findings of these studies, similar to those obtained in Khezr, point to a common set of issues affecting communities in both rural and urban settings.
Additional studies have identified similar patterns across Iran. For example, Karimi et al identified drinking water contamination, economic hardships, unemployment, lack of awareness of medical issues, tobacco use, hypertension, sedentary lifestyles, high-risk behaviors among adolescents, and insufficient consumption of fruits and vegetables as key issues in Cheliche, located in Chaharmahal and Bakhtiari province (3). Mokhtari et al conducted research in Azarshahr, highlighting the top ten problems in that region, including depression, unemployment, unsanitary garbage collection and sewage disposal, forced marriages of girls, lack of recreational and sports spaces, narrow streets, stray dogs, underutilization of natural resources, and inadequate health and treatment facilities (18). In Shahinshahr (Isfahan), Karimi et al reported drug use, smoking, poverty, unemployment, housing problems, depression, youth violence, stroke, and lung cancer as major issues (5). These studies all share common themes of economic difficulties, mental health issues, unemployment, and lack of healthcare access, demonstrating how intertwined these issues are with the broader health landscape of various regions.
The differences between the findings related to the Khezr region and other regions are likely rooted in the unique cultural, economic, and social conditions present in this region. Each community faces its own distinct set of challenges, making localized assessments like this one crucial for understanding and addressing region-specific needs. Conducting a localized needs assessment allows for the development of tailored interventions that directly respond to the community’s most pressing issues. Despite regional differences, there are consistent underlying factors—such as poverty and lack of social support—that are common across various studies. Addressing these root causes is essential to improving overall community health and well-being.
Poverty, as the most significant problem identified in this study, affects all aspects of life in the Khezr region. Economic hardship exacerbates existing health problems, limits access to necessary healthcare, and contributes to a lower overall quality of life. Given the widespread effects of poverty, addressing this issue must be a top priority for both local and national authorities. Effective strategies to reduce poverty will require coordinated efforts across multiple sectors, including health, education, and economic development. Without comprehensive intervention, the well-being of the Khezr region’s population will continue to suffer, perpetuating cycles of poor health and diminished opportunities for social and economic advancement.
This study faced several limitations, which were anticipated at the outset. One challenge was the reluctance of many local residents to participate, driven by a belief that such research would not lead to meaningful changes. Additionally, low literacy levels in the region presented difficulties in communication and accurate data collection from some participants. Recent migration into the area further complicated data collection, as newcomers were often less familiar with the long-standing issues affecting the region. Another limitation of our study was the small sample size, which was due to financial and time constraints that prevented the collection of a larger sample. Despite these obstacles, the study succeeded in identifying poverty (low income) as the most critical issue facing the Khezr region. This was unanimously expressed by both residents and local officials, underscoring the profound impact of economic hardship on personal health, quality of life, and access to healthcare services.
Conclusion
The study of the Khezr region revealed significant challenges, including widespread poverty, high unemployment, inadequate healthcare access, and public health issues (e.g., addiction, mental health disorders, and chronic diseases). Poverty and unemployment emerged as the most pressing concerns, impacting the quality of life and requiring urgent intervention. Community dissatisfaction with health services, safety concerns, and limited emergency preparedness further highlighted the region’s vulnerabilities. Addressing these issues calls for targeted economic development, healthcare improvements, and enhanced education and preventive care services. Collaborative, sustainable strategies are essential for improving living conditions and fostering resilience in the community.
Acknowledgments
The authors would like to acknowledge the valuable contributions of the staff of the Health Center of the Khezr Region, who provided essential assistance and support during the data collection phase of this study.
Authors’ Contribution
Conceptualization: Sanaz Omidi, Mehdi Mousavi, Younes Mohammadi.
Data curation: Reza Bigdeli.
Formal analysis: Sanaz Omidi.
Investigation: Mansour Salehpour, Zahra Yazdanian, Parham Mohammadi, Saber Ghaffari, Abouzar Raeisvandi.
Methodology: Sanaz Omidi, Mansour Salehpour, Zahra Yazdanian, Parham Mohammadi, Saber Ghaffari, Abouzar Raeisvandi.
Supervision: Reza Bigdeli, Mehdi Mousavi, Younes Mohammadi.
Visualization: Sanaz Omidi.
Original-draft writing: Sanaz Omidi, Younes Mohammadi.
Writing-review & editing: Mansour Salehpour, Reza Bigdeli, Zahra Yazdanian, Parham Mohammadi, Mehdi Mousavi, Saber Ghaffari, Abouzar Raeisvandi.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
The study has received approval from the Ethics Committee of Hamadan University of Medical Sciences (reference No. IR.UMSHA.REC.1403.853).
Funding
This research was supported by Hamadan University of Medical Sciences (1403112310156). The funders had no role in the design, data collection, analysis, or interpretation of the data or manuscript writing.
References
-
Eaton SA. Using the Community Health Assessment (CHA) to Reduce Racial Health Disparities within Gaston County’s African American Population. University of North Carolina at Chapel Hill; 2018. doi: 10.17615/vea8-5z37.
- Holakouie-Naieni K, AhmadiPishkuhi M, Shafieezadeh T, Salehiniya H, Pooya B. Review the Results of the Community Assessment Projects in Areas Covered by Health Centers in Iran During the Years 1992-2013. Iranian Journal of Epidemiology 2015; 11(2):69-82. [ Google Scholar]
- Abbasi-Ghahramanloo A, Safiri S, Torkamannezhad-Sabzevari J, Kogani M, Holakouie Naeini K, Hassanipour Azgomi S. Community assessment for identification and prioritization of health problems in Navai Kola village, Babol, Iran. Journal of Analytical Research in Clinical Medicine 2016; 4(1):47-54. doi: 10.15171/jarcm.2016.008 [Crossref] [ Google Scholar]
- Rahmani K, Holakouie-Naieni K, Moradi G. Utilization of community assessment model for identification of family health problems. J Sabzevar Univ Med Sci 1970;21(6):1035-44. [Persian].
- Karimi J, Holakouie-Naieni K, Ahmadnezhad E. Community assessment of Shahin-Shar, Isfahan, IR Iran to develop community health action plan. Iran J Epidemiol 2012;8(1):21-30. [Persian].
- Basseej MH, Holakouie-Naieni K, Ardalan A, Ahmadnezhad E. Community Assessment for Determining the Health Priority Problems and Community Diagnosis: A Case Study of Qala_Sayed Village, Kazeroun, Fars Province, Iran. Iran J Public Health 2015; 44(9):1303-5. [ Google Scholar]
- Maleki f, Hosseinpour M, Rafiemanesh H, Salehi F, Lotfi Z, Naserizadeh MR, et al. The review of community assessment papers to determine priority problems in selected populations of Iran. Journal of School of Public Health & Institute of Public Health Research 2015;12(3):13-21. [Persian].
- Rafiemanesh H, Yari M, Khodabakhshi Nejad V, Holakouie-Naieni K. Community assessment for determination and diagnosis of health-related problems in Aliny village Meshginshahr functions in Ardebil. J Prevent Med 2015;2(2):10-7. [Persian].
- Cottler LB, Nagarajan R. Real-time assessment of community health needs and concerns. Sci Transl Med 2012; 4(119):119mr2. doi: 10.1126/scitranslmed.3003367 [Crossref] [ Google Scholar]
- Madani A, Shekari M, Nejatizadeh A, Aghamolaei T, Azarpakan A, Holakouie-Naieni K. Community assessment to identify and prioritize problems of Hormoz island, in the south of Iran. J Prevent Med 2015;2(4):58-70. [Persian].
- Ardalannejad S, Naeimi A, Badsar M. Analyzing the effect of community-based addiction prevention plan on the quality of life of Marivan county villagers. J Rural Res 2022; 12(4):816-31. doi: 10.22059/jrur.2021.311907.1568.[Persian] [Crossref] [ Google Scholar]
- Mohammadi Y, Javaheri M, Mounesan L, Rahmani K, Holakouie-Naieni K, Madani A, et al. Community assessment for identification of problems in Chahestani region of Bandar-Abbas city. Journal of School of Public Health & Institute of Public Health Research 2010;8(1):21-30. [Persian].
- Rahmani K, Holakouie-Naieni K, Moradi G. Utilization of community assessment model for identification of family health problems. J Sabzevar Univ Med Sci 1970;21(6):1035-44. [Persian].
- Shekari F, Jalilvand H, Mohammadpoorasl A. Community health assessment to identify problems and develop operational plans to promote health in the Soufian district. Journal of School of Public Health & Institute of Public Health Research 2022;20(2):143-56. [Persian].
- Karimi Z, Hamid K, Safi K, Pasdar Yazd M, Mohammadian-Hafshejani A. Community health assessment for identifying and prioritizing the problems of Choliche county, Farsan city, Chaharmahal and Bakhtiari province, Iran. J Prevent Med 2023; 10(2):148-61. doi: 10.32598/jpm.10.2.576.1.[Persian] [Crossref] [ Google Scholar]
- Holakouie-Naieni K, Karimi J, Karimi R. Community Health Assessment Guide. Rasht: Gap; 2018. [Persian].
- Keykavoos Iranag M, Pashapour H, Jafari A, Keshavarzian K, Khodamoradi M, Dorosti AA, et al. Community health assessment of the town of Basmenj, Tabriz city. Journal of School of Public Health & Institute of Public Health Research 2018;16(3):295-306. [Persian].
- Mokhtari M, Banaye Jeddi M, Majidi A, Jafari Khoenagh A, Holakouie-Naieni K. Community assessment for identification and prioritization of problems to establish health promotion operational plans. Journal of Research and Health 2013;3(1):295-302. [Persian].