J Educ Community Health. 12(2):77-84.
doi: 10.34172/jech.3136
Original Article
Uncovering the Complexities of HIV Care: A Qualitative Study on Adherence and Prevention in Urban South Gujarat, India
Manvendra Singh Rathore Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, 1 
MohamedAnas MohamedFaruk Patni Data curation, Formal analysis, Software, Visualization, Writing – original draft, 2
Samudyatha UC Data curation, Investigation, Visualization, Writing – review & editing, 3
Jayendrakumar Kosambiya Conceptualization, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing, 4, *
Rajesh Gopal Funding acquisition, 5
Author information:
1Department of Community Medicine, Government Medical College, Surat, India
2Department of Community Medicine, RAK College of Medical Sciences, RAK Medical and Health Science University, Ras Al Khaimah, United Arab Emirates
3Department of Community Medicine, Sri Devaraj Urs Medical College, Kolar, India
4Department of Community Medicine, Kiran Medical College, Surat, India
5Gujarat State AIDS Control Society, Gujarat, India
Abstract
Background: The perception of HIV within the scientific community and the public has evolved from considering it a "life-threatening fatal disease" to viewing it as a "chronic manageable disease." This study examined the evolving landscape of HIV treatment and prevention within the framework of the Test and Treat Policy. It explored factors contributing to HIV infection and the challenges related to treatment adherence among newly infected patients living with HIV (PLHIV) and PLHIV who have been lost to follow-up (LFU) in an urban setting.
Methods: This qualitative study was conducted at an ART Centre in a tertiary care hospital in South Gujarat. The participants included 20 male PLHIV, 10 newly infected individuals and 10 who had been LFU. Purposive sampling was employed to select participants based on specific criteria, including enrolment at the ART Centre after April 2017 and a willingness to provide informed consent. In-depth interviews (IDIs) were conducted, and audio recordings were translated, coded, and analyzed using thematic analysis in Atlas Ti software to identify key themes related to HIV infection and challenges in treatment adherence.
Results: Thematic analysis identified several key themes. Among newly infected participants, long-term high-risk sexual behaviors and isolated incidents of unprotected sex were significant contributors to HIV acquisition. In the LFU group, economic constraints such as wage loss and lack of financial support, were major reasons for missed ART visits. Fear of discrimination in workplace and within the family, compounded by insufficient family support, further hindered adherence. Some participants expressed feelings of hopelessness, leading to ART discontinuation.
Conclusion: Addressing high-risk behaviours, socio-economic challenges, and stigma is crucial to improving HIV prevention, treatment adherence, and overall health outcomes among newly infected PLHIV in urban areas.
Keywords: HIV treatment, Test and treat policy, Qualitative study, Treatment adherence, Economic barriers
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Rathore MS, Patni MM, UC Samudyatha, Kosambiya J, Gopal R. Uncovering the complexities of HIV care: a qualitative study on adherence and prevention in urban south Gujarat, India. J Educ Community Health. 2025; 12(2):77-84. doi:10.34172/jech.3136
Introduction
The perception of HIV within the scientific community and the public has shifted from considering it a “life-threatening fatal disease” to viewing it as a “chronic manageable disease.” Since the detection of the first cases of HIV, the management and treatment of HIV have also evolved, from mere supportive therapies to the currently accepted “Test and Treat Policy.” Recommended by the World Health Organization (WHO) in 2016, the policy advocates initiating antiretroviral treatment (ART) for all HIV-positive individuals irrespective of the CD4 count to reduce the viral load to an “undetectable” level and thereby minimizing the risk of transmission (1).
Although the policy is grounded in strong scientific evidence supporting its clinical effectiveness (2-5), its application in resource-limited environments such as India encounters numerous challenges. Although the policy seeks to reduce transmission rates and enhance treatment outcomes, adherence issues persist among newly infected people living with HIV (PLHIV) and those lost to follow-up (LFU) (6). Earlier studies have identified economic, social, and psychological barriers to adherence, including stigma and discrimination, as well as the social determinants of health(7). However, qualitative research has not extensively addressed the lived experiences of PLHIV in urban settings, where socioeconomic inequalities and mobility significantly affect treatment continuity.
In the Indian context, the application of the Test and Treat Policy overlaps with social issues, including stigma, healthcare availability, and socio-economic issues (8,9). The enactment of the HIV/AIDS Prevention and Control Act of 2017 intended to safeguard the rights of PLHIV; however, social stigma and adherence-related challenges continue to be major obstacles (10). Moreover, the legalization of same-sex relationships in 2018 introduced a new dimension to the multifaceted social issues impacting ART adherence (11).
Lacking sufficient experiences of PLHIV in urban settings in India, the present research addressed an important knowledge gap. Although the prevalence of non-adherence and LFU among PLHIV has been well documented using quantitative data, there is limited qualitative information on the underlying reasons for these issues from the patient’s perspectives. Developing effective intervention programs targeting both structural and patient barriers requires an understanding of these lived experiences.
This research was designed to investigate the determinants of HIV infection and the barriers to ART adherence among newly diagnosed PLHIV and LFU cases in an urban context in South Gujarat. Focusing on the contextual realities and lived experiences of affected individuals, the research strived to inform more context-specific and patient-centric healthcare interventions.
Materials and Methods
Study Design and Setting
This qualitative study used an inductive thematic analysis approach to explore the factors influencing HIV infection and challenges related to ART adherence among newly infected PLHIV and those identified as LFU in an urban context. The study was conducted at an ART Centre in a tertiary care hospital located in South Gujarat, India. The study was conducted at an ART Centre in a tertiary care hospital located in South Gujarat, India. The study was designed to gain in-depth insights into the lived experiences of PLHIV through qualitative methods, with a focus on thematic analysis.
Participant Selection and Sampling Strategy
Participants were selected through purposive sampling based on predefined eligibility criteria. A list of eligible individuals was generated through a desk review of ART Centre records. Participants included 20 male PLHIV, divided into two groups:
-
Group 1: 10 men recently diagnosed with HIV. The demographic profile of newly infected participants is presented in Table 1.
-
Group 2: 10 men LFU or missed ART appointments. Table 2 provides the demographic details of the missed and loss to follow-up participants.
Table 1.
Profile of “Newly Infected Male” Participants
|
IDI
|
Age (years)
|
Marital Status
|
Migration
|
Education
|
Occupation
|
Socio-economic Status Based on Income Level, Occupation, and Education
|
| IDI 1 |
30 |
Married |
No |
Graduate |
Business |
II |
| IDI 2 |
31 |
Married |
No |
Secondary |
Landholder |
IV |
| IDI 3 |
21 |
Single |
Yes (Uttar Pradesh) |
Primary |
Service |
II |
| IDI 4 |
33 |
Re-Married |
No |
Primary |
Skilled Worker |
II |
| IDI 5 |
50 |
Married |
No |
Primary |
Skilled Worker |
III |
| IDI 6 |
37 |
Married |
Yes (Uttar Pradesh) |
Secondary |
Skilled Worker |
III |
| IDI 7 |
33 |
Married |
Yes (Uttar Pradesh) |
Primary |
Business |
I |
| IDI 8 |
41 |
Married |
Yes (Uttar Pradesh) |
Secondary |
Local Transport Worker |
IV |
| IDI 9 |
39 |
Married |
No |
Secondary |
Local Transport Worker |
II |
| IDI 10 |
28 |
Single |
Yes (Maharashtra) |
Secondary |
Laborer |
II |
Table 2.
Profile of Participants Selected as “Missed” or “Loss to Follow up”
|
IDI
|
Age (years)
|
Gender
|
Migration
|
Education
|
Occupation
|
Socio-economic Status
|
| IDI 11 |
30 |
Male |
No |
Primary |
Skilled Worker |
II |
| IDI 12 |
43 |
Male |
No |
Primary |
Unemployed |
IV |
| IDI 13 |
37 |
Transgender/ Transsexual |
Yes (Maharashtra) |
Graduate |
Service |
I |
| IDI 14 |
40 |
Male |
Yes (Maharashtra) |
Primary |
Service |
II |
| IDI 15 |
34 |
Male |
Yes (Nepal) |
Primary |
Service |
III |
| IDI 16 |
30 |
Female |
No |
Secondary |
Skilled Worker |
I |
| IDI 17 |
43 |
Male |
Yes (Uttar Pradesh) |
Secondary |
Service |
I |
| IDI 18 |
37 |
Female |
No |
Primary |
Laborer |
IV |
| IDI 19 |
40 |
Female |
No |
Secondary |
Skilled Worker |
V |
| IDI 20 |
34 |
Male |
No |
Secondary |
Laborer |
II |
Note: Education levels based on the Indian education system: Primary: Up to Grade 7; Secondary: Grade 10 up to Grade 10; High secondary: Grade 11 and grade 12; Graduate: Bachelor’s Degree.
Inclusion criteria required participants to be male PLHIV enrolled at the ART Centre after April 2017, either newly infected or reinitiated on treatment after being classified as LFU or missed. Additionally, participants had to be over 18 years of age, willing to give consent, and attending the ART Centre in a tertiary care hospital in South Gujarat. Newly infected female PLHIV were excluded due to operational and cultural challenges in engaging newly diagnosed women in in-depth interviews (IDIs) within the given setting. Access to newly diagnosed female PLHIV was limited due to social norms and privacy concerns, which made recruitment and data collection challenging.
Data Collection
Data were gathered from IDIs administered in Hindi and Gujarati by trained investigators. IDIs explored participants’ opinions on HIV acquisition, treatment adherence, and related social issues. It was piloted with two participants from similar backgrounds to test for clarity, relevance, and cultural appropriateness. Based on the pilot feedback, minor adjustments were made to the phrasing and sequence of questions to enhance participant comfort and data richness. Interviews were audio-recorded with participant consent and supplemented by field notes. Interview length varied from 30 to 60 minutes based on participant engagement and cooperation. To have accurate data, the recordings were transcribed word for word and translated into English. Transcripts were checked for research consistency and accuracy by an independent researcher (Figure 1).
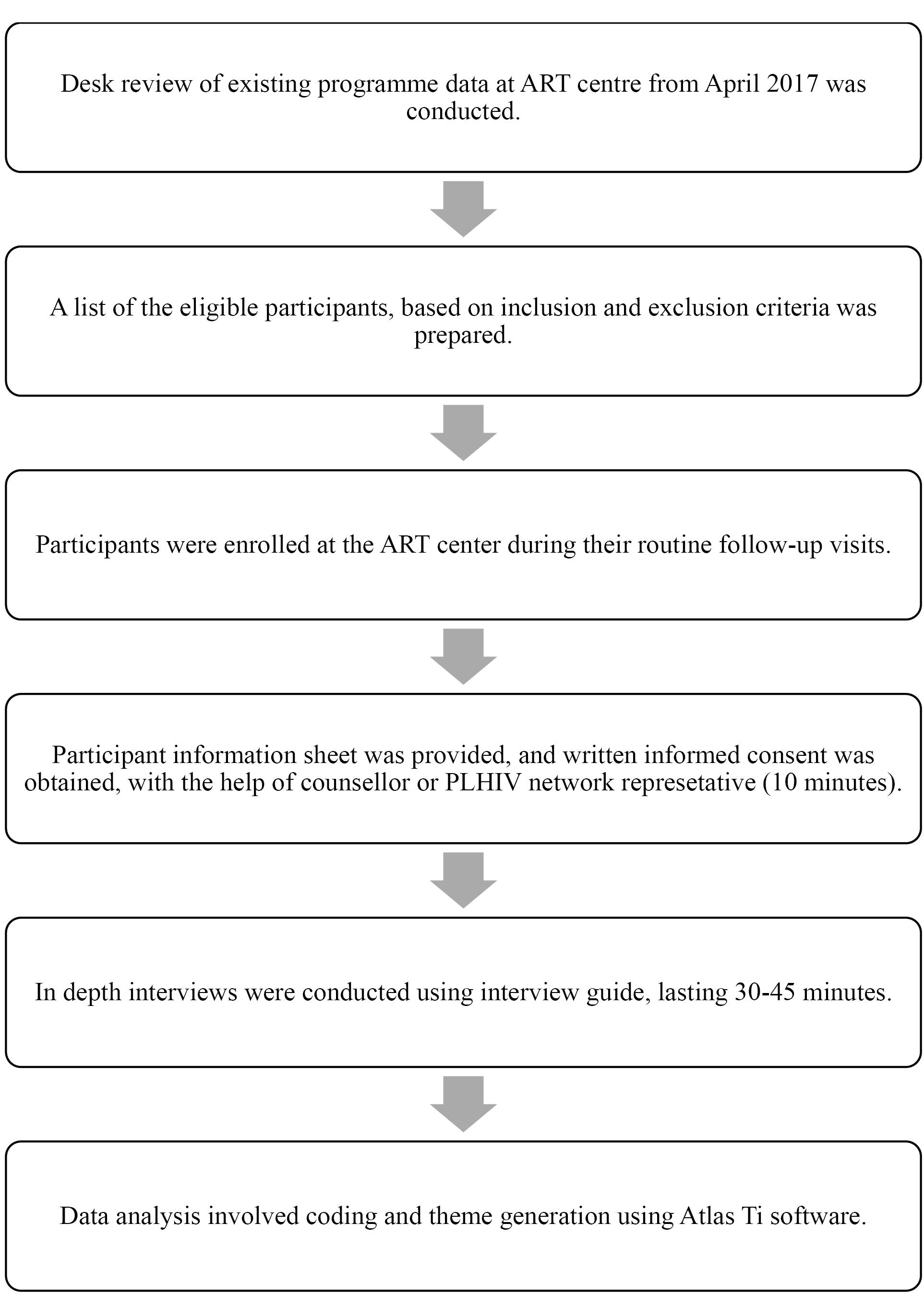
Figure 1.
Flowchart of the Study
.
Flowchart of the Study
Data Analysis
Thematic analysis was used to identify recurring patterns and key themes, with the translated transcripts coded using Atlas Ti software following six steps: 1) familiarization with data through repeated reading of transcripts, 2) generating initial codes by identifying meaningful data segments, 3) searching for themes by grouping similar codes, 4) reviewing themes to refine and merge them, 5) defining and naming themes with clear articulation, and 6) producing the final report by synthesizing the findings. The codes and themes were cross-verified by multiple researchers, to ensure consistency and reliability.
Definitions Used
-
Newly infected male PLHIV: Those male PLHIV who have been newly enrolled at ART Center with a baseline CD4 count ≥ 700.
-
Missed: Those participants who had missed less than three visits after ART initiation.
-
LFU: Those who had returned to treatment after missing three or more than three consecutive visits after ART initiation.
Data Trustworthiness and Validity
The research employed the following practices to ensure the accuracy and reliability of the findings:
-
Credibility: We employed triangulation by comparing the responses of various participants and requested some of the participants to confirm the accuracy of what we interpreted (member checking).
-
Dependability: The steps of data collection and coding were well documented in order to be consistent and cross-checked by multiple researchers.
-
Confirmability: The researchers maintained reflective journals to be mindful of their own biases, and coding discrepancies were discussed and resolved by the research team.
-
Transferability: We provided detailed descriptions of the setting and participants to enable the applicability of the findings to similar contexts.
Results
Themes Generated From In-Depth Interviews of “Newly Infected Male” Patients Living With HIV
Long-term High-Risk Sexual Behaviour Before Diagnosis
Participants described high-risk sexual behavior such as having unprotected sexual activity with a person of unknown status for a long time. In one case the interviewee described how he was a regular client for commercial sex work.
“I am 41 and still unmarried. My friends and relatives of the same age have grown-up children. I have struggled to maintain relationships on which I could build my life. So yes, sometimes I visit a known place in the east of the city to find some relief.” (IDI 8)
Sometimes, the geographical location was far off, in another city or state, such as in the case of IDI 3:
“After testing positive, I researched the possible routes of transmission. I realized it was probably the physical (sexual) route in my case. I will not hide it as there is no point hiding it. I used to visit Daman every weekend. There I met people and paid encounters.” (IDI 3)
In another instance, the interviewee had two fixed partners over a period of time at different places. He described his experience as follows:
“I used to have two partners one male in the city and one female in my native village. My last time contact with a female partner was almost a year ago, while with a male partner, it was seven months back. The male partner got tested right after my diagnosis. I lost touch with my female partner, and I actually don’t know what happened to her.” (IDI 10)
Isolated incidents of high-risk behavior
In some cases, the individuals were not engaged in prolonged high-risk behaviors but reported isolated incidents, which likely resulted in their acquiring HIV infection. Movements of people across borders for livelihood and recreation led to infections occurring elsewhere, as in the case of IDI 6:
“It was more than 6 years since I last visited my home. During this festival season, I went to my native village where other childhood friends who work in other states were also there. My close childhood friend told me that he knows a place where we can go and relax.” (IDI 6)
However, in the case of IDI 5, it was a misunderstanding of how HIV spreads that led him to indulge in high-risk sexual activity with a false sense of safety.
“I went to my friend’s son’s marriage. They had arranged for such activities at the place where we stayed, and I had it. I never went to the place where they (sex workers) live. I thought that the infection only spreads if we go to their homes for activity.” (IDI 5)
In some instances, the isolated incident of unprotected sexual activity occurred in the city itself, such as in the case of IDI 2:
“I was sent to the eastern part of the city for some training by my employers. After the training session, I went to the home of a colleague who is a local resident, and there he had arranged some women whom we can pay and relax.” (IDI 2)
Infection Acquired From the Infected Female Partner
In some cases, the interviewees recalled how they were unaware of their wives’ HIV-positive status until they themselves were diagnosed.
In the case of IDI 4, there was a missed opportunity for earlier detection, which might have prevented the spread to his second wife.
“This is my second marriage. My first marriage didn’t last long. Soon after my first marriage, my wife was admitted and died in a private hospital. This happened so fast, within less than one year, that I didn’t understand what happened to her. All we were told was that there was some serious lung infection which had spread to the brain, which killed her. Then, I got married again, and my second wife tested positive when she was pregnant. I brought the old hospital records here to the ART center and was explained that my first wife had been infected. Her parents were on ART too, for 12 years and taking medication here. Nobody told me – neither her parents nor her doctors.” (IDI 4)
In the case of IDI 7, repeated tests conducted at various fertility clinics during the early years of their marriage showed that neither IDI 7 nor his wife were HIV positive. However, an HIV test performed in the seventh year of their marriage revealed that both were infected.
“There was a time when my wife’s parents asked me to send her to the village so they could take her to some spiritual center that helps women conceive. After being tested positive, I questioned my in-laws about where or to whom they had taken my wife for treatment. They told me about some sort of fraudulent yogi in their village who runs this spiritual center and treats everyone and everything with his magical needle. Who knows what else he does?” (IDI 7)
Themes Generated From In-Depth Interviews of “Missed” Patients Living With HIV
IDIs with patients who missed their ART visits in the past year exhibited three major themes for missed visits: financial problems, fear of discrimination, and lack of family support. An additional theme was the struggle to hide one’s HIV-positive status.
Economic and Social Barriers
Among daily wage workers employed temporarily, fear of losing wages prompted them to miss clinic visits, as in the case of IDI 11.
“Yes, I didn’t come to the ART center for one month and completely missed my medicines for that month. I work as a textile power loom operator, and I am paid hourly - if I have an eight-hour shift and work for six hours only, I will get paid for six hours only. I did not want to lose that money. That is why I did not come.” (IDI 11)
In other cases, such as IDI 12, receiving ART was not a priority at all due to the absence of a fixed income or financial support:
“I have been jobless for the last year. I don’t have any income. I somehow manage daily expenses with help from my brother. It is with this money that I buy food. Sometimes I do not even have money for food, so how will I get money for bus fare to come here? When I was linked to this ART center, I was promised monthly financial assistance. I have submitted all the required documents, but to date, not a single rupee has been credited to my account.” (IDI 12)
Additionally, the fear of wage loss was often compounded with the fear of loss of work itself if the employers were to discover their status, as in the case of a transgender participant:
“I have missed two appointments in the last year. Tell me - in this society, who will give jobs to people like me? Now, I have managed to get one, and I don’t want to lose it. I don’t want this disease to cost me my job. Hence, sometimes situations arise at work when I am unable to visit the ART center on the scheduled date.” (IDI 13)
Fear of Discrimination
Participants reported missing visits to the ART center due to fear of revealing their HIV status at work because they were worried about job loss and discrimination at workplace. For example, IDI 11 felt that concealing his positive status was necessary:
“My employer is from a very orthodox family, and he is a strict and religious person. He simply won’t be able to accept my condition, my illness. I will lose my job if he finds out about my status, and he will make sure that I never get a job anywhere in the city. It is not only about the job... I have over ten years of experience working with power looms and hold a respectable position among my colleagues, too! What will happen if they find out about my status? Therefore, it is better to lose wages than respect and job, isn’t it?” (IDI 8)
Some, like IDI 14, feared stigma from his family, if they were to learn about his positive status.
“After missing my appointment, staff from the ART center contacted me and asked if I wanted them to visit my family. This was unacceptable to me, so I decided to tell my employer that I had been diagnosed with a kidney infection and had to go to a government hospital monthly for checkups. Since then, I have continuously adhered to my treatment without missing any single appointment.” (IDI 14)
Lack of Family Support
Among migrant participants, who shared accommodation with other migrant workers, the fear of stigma from members of the household and lack of family support was evident, as in the case of IDI 15:
“I am currently sharing an apartment with my colleague. We work and live together. If I tell them that I have this infection, they will leave me, and I might lose my job as well. Even if I do not lose my job, what about the accommodation? I cannot afford a single accommodation, as I have to send money home, too! I get help from my neighbor who sometimes lends me money, but I can’t tell him either, because he is the only person who helps me from time to time. What if he finds out about my infection and stops helping or talking to me? I just can’t afford that!” (IDI 15)
These participants, in fact, struggled in various ways, to conceal their identity at both their work and home, as in the case of IDI 13.
“I somehow managed to convince my employer that I have to visit Devi’s temple once a week. Based on my ART appointment scheduled, I go to the temple for three weeks and to the ART center in the fourth week.” (IDI 13)
Healthcare System Barriers
In another instance, a participant employed in a traveling job described how a miscommunication with the ART center resulted in a three-month interruption in his treatment. He was unable to inform the center that he would be leaving town for a work-related assignment and consequently did not collect his medication in advance. He was also unaware of the provision allowing PLHIV with good adherence and stable health to receive a longer duration of medication.
“I worked in the catering business as a staff manager. A few months ago, my boss suddenly informed us that our team had to go to Dubai within a week, as he had got some big orders for an exhibition there. Due to the scarcity of time and a heavy workload, I could not visit the ART center to inform them about my travel. In the meantime, I was also afraid that the doctor might not allow me to go abroad for such a long period. At that time, I certainly could not afford to miss this opportunity to earn money.” (IDI 20)
The participants described how the ART staff repeatedly reached out to them to convince them to reengage in ART:
“After I stopped visiting the ART center, I started getting phone calls from them, which I initially avoided. Later, the staff came to our house and convinced me to restart the treatment- if not for myself, then at least for my child.” (IDI 18)
As in the case of IDI 16, ill health prompted the LFU to come back and restart ART, “Then, I was severely ill. I had to come to the hospital and take medicines. They told me to take these medications, too. When I have so many other medicines to take, why leave out these? So, I started taking them as well.”
Feeling of hopelessness
Participants LFU and later returned to the ART center described a fine balance between the reasons to stop ART and restarting treatment. Among the most profound reasons for stopping ART was the feeling of hopelessness. These participants also faced other personal issues such as the lack of family support, as in the case of IDI 16:
“My husband left me five years ago. I have nobody in my life. About two years ago, I developed urinary problems and was diagnosed with HIV. I have been on ART since then. The urinary issues gradually resolved, but I have developed continuous nausea ever since. It feels like when one problem is solved, another comes up. I keep asking myself, what is left in my life? My husband left me for another woman, I have no children. The male partner I had stopped treating me the same way as he used to. To be honest, I am currently taking the medicines because the doctor advised me. I think that taking medicines regularly is not helpful as my reports and CD4 counts are not improving. This is my story, and I hope that it is evident why I missed my ART appointments for three months in a row.” (IDI 16)
Discussion
The evolution of HIV from a “life-threatening fatal disease” to a “chronic manageable disease” has dramatically altered both public perception and the medical management of HIV.
Our research found fear of workplace discrimination as one of the primary reasons for missed ART appointments among migrant workers and day-wage workers. Participants were worried about losing their jobs and becoming socially ostracized if their HIV status were disclosed. This finding aligns with Basu et al (12) who documented stigma as a major barrier to ART adherence among PLHIV. Similarly, Ekstrand et al (13) noted that stigma not only impedes adherence but also negatively affects the overall quality of life of HIV-infected people in rural India. In the present research, stigma was particularly acute among migrant workers who lacked support networks and were at risk of losing both employment and housing.
Economic barriers also contributed significantly to treatment interruption. Participants who worked in informal or unstable sectors reported losing a day’s wages by attending appointments at the ART center, which directly impacted their families’ financial well-being. This was particularly pronounced among migrant workers who were more susceptible to economic instability. Our findings align with Bandyopadhyay et al (14) who reported a strong relationship between economic insecurity and non-adherence to ART. Similarly, Surti et al (15) found that sex workers experienced heightened risks of sexually transmitted infection due to economic pressures and inconsistent condom use- risks further compounded by exposure to violence. In the Indian context, where most PLHIV earn low wages through informal work, even minor disruptions to income can have serious implications. Economic vulnerability must be addressed not just through enhanced healthcare access but also through broader policy interventions aimed at promoting economic stability among PLHIV.
Another significant finding was the psychological distress associated with HIV, with several participants expressing feelings of hopelessness regarding their treatment. This was generally attributed to the perception that the treatment did not seem to yield tangible health improvements for some individuals who questioned its worth. These attitudes reflect the dynamic interaction between treatment adherence and mental health, as highlighted by Islam et al (16), who showed that depression and anxiety can significantly hamper adherence to ART. Integrating mental health services into the ART programs would help address such concerns and improve adherence outcomes.
Our research also revealed that transgender individuals (TG/TS) face special challenges related to both HIV and gender stigma. Social acceptance has not changed much despite the decriminalization of same-sex relationship in 2018 (17-19). Participants felt excluded from visiting ART centers, where at times doctors did not respond sensitively to their particular circumstances. UNAIDS has highlighted that while laws may change for transgender people, this does not necessarily reflect better attitudes in healthcare or reduced stigma (20). In Southern Gujarat, where HIV status intersects with gender identity, it creates extra barriers to treatment adherence.
Healthcare barriers also manifested in logistical concerns, including the distance to ART facilities, lengthy wait times, and inflexible hours of operation. Individuals with long work hours or field assignments often had trouble keeping appointments on time. Misunderstanding between healthcare workers and clients regarding prescription refills while traveling also contributed to treatment interruptions. This mirrors findings from other studies (21,22), which identified infrastructure-related barriers in healthcare as limiting adherence in settings with limited resources. Enhanced patient-provider communication and multi-month dispensing of ART can possibly address these issues.
In short, our research highlights the necessity of culturally appropriate, multi-faceted interventions targeting economic, social, and psychological barriers to ART adherence among PLHIV in Southern Gujarat. These findings underscore the need for more adaptive healthcare models with economic support, mental health services, and stigma reduction. Community-level outreach activities, coupled with strengthened training of healthcare providers, can have a strong impact on adherence and overall health outcomes in marginalized settings.
The study has a few limitations, including the exclusive focus on male PLHIV, which limits generalizability, and the qualitative design, which, while providing rich insights, may not capture the full diversity of experiences. Conducted in a single ART center in South Gujarat, the findings may not be representative of other regions.
Conclusion
Although the Test and Treat Policy has augmented ART coverage, it is essential to overcome the socio-economic and psychological barriers unique to Southern Gujarat to help people maintain adherence. Our research identifies the need for context-specific interventions that address the specific challenges faced by migrant workers, transgender people, and workers in the informal economy. The inclusion of mental health care, economic support, and stigma reduction in ART programs can enhance health outcomes and augment the ultimate objective of eradicating the AIDS epidemic.
Competing Interests
None declared.
Ethical Approval
Ethical approval was obtained from the Human Research and Ethics Committee (No. MCS/STU/ETHICS/PERMISSION/13148/19, dated 24 May 2019). Written informed consent was obtained from all participants prior to data collection. Participants were assured of confidentiality, and pseudonyms were used to protect their identities. Data were securely stored with access limited to authorized research personnel.
Funding
The study was funded by Indian Council of Medical Research with letter No. 3/2/March-2019/PG-Thesis-HRD (31)/Dated: 25-03-2019.
References
- Joint United Nations Programme on HIV/Aids (UNAIDS). 90-90-90: An Ambitious Treatment Target to Help End the AIDS Epidemic. United Nations; 2014. p. 10-5. Available from: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf.
- Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med 2016; 375(9):830-9. doi: 10.1056/NEJMoa1600693 [Crossref] [ Google Scholar]
- Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med 2012; 367(5):399-410. doi: 10.1056/NEJMoa1108524 [Crossref] [ Google Scholar]
- Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med 2012; 367(5):423-34. doi: 10.1056/NEJMoa1110711 [Crossref] [ Google Scholar]
- Das M, Chu PL, Santos GM, Scheer S, Vittinghoff E, McFarland W. Decreases in community viral load are accompanied by reductions in new HIV infections in San Francisco. PLoS One 2010; 5(6):e11068. doi: 10.1371/journal.pone.0011068 [Crossref] [ Google Scholar]
- Hossain F, Hasan M, Begum N, Mohan D, Verghis S, Jahan NK. Exploring the barriers to the antiretroviral therapy adherence among people living with HIV in Bangladesh: a qualitative approach. PLoS One 2022; 17(10):e0276575. doi: 10.1371/journal.pone.0276575 [Crossref] [ Google Scholar]
- Nair M, Kumar P, Pandey S, Harshana A, Kazmi S, Moreto-Planas L. Refused and referred-persistent stigma and discrimination against people living with HIV/AIDS in Bihar: a qualitative study from India. BMJ Open 2019; 9(11):e033790. doi: 10.1136/bmjopen-2019-033790 [Crossref] [ Google Scholar]
- Singh SK, Shri N. Sociodemographic correlates of discrimination against PLHIV in high HIV prevalence states of India, NFHS 2016-21. Sci Rep 2023; 13(1):15083. doi: 10.1038/s41598-023-42162-6 [Crossref] [ Google Scholar]
- Lodge W 2nd, Chaudary J, Rawat S, Agénor M, Dange A, Anand VR. From policy to practice: syndemic and intersectional challenges to ART adherence for transgender women under India’s post-test and treat policy. Glob Public Health 2025; 20(1):2473446. doi: 10.1080/17441692.2025.2473446 [Crossref] [ Google Scholar]
- Ministry of Law and Justice (Legislative Justice). The HIV and AIDS (Prevention & Control) Act, 2017 [Internet]. India: Ministry of Law and Justice; 2017. p. 16. Available from: https://naco.gov.in/sites/default/files/HIV%20AIDS%20Act.pdf.
- Bhutada K, Chakrapani V, Gulfam FR, Ross J, Golub SA, Safren SA. Pathways between intersectional stigma and HIV treatment engagement among men who have sex with men (MSM) in India. J Int Assoc Provid AIDS Care 2023; 22:23259582231199398. doi: 10.1177/23259582231199398 [Crossref] [ Google Scholar]
- Basu S, Marimuthu Y, Garg S, Saravanakumar V, Ganesh B. Anti-retroviral therapy adherence in India (2012-18): a systematic review and meta-analysis. Indian J Sex Transm Dis AIDS 2024; 45(1):2-7. doi: 10.4103/ijstd.IJSTD_28_20 [Crossref] [ Google Scholar]
- Ekstrand ML, Heylen E, Mazur A, Steward WT, Carpenter C, Yadav K. The role of HIV stigma in ART adherence and quality of life among rural women living with HIV in India. AIDS Behav 2018; 22(12):3859-68. doi: 10.1007/s10461-018-2157-7 [Crossref] [ Google Scholar]
- Bandyopadhyay A, Chaurasia RC, Palepu S, Yadav RK. A study of adherence to antiretroviral therapy in a tertiary care hospital at Allahabad, India. Indian J Sex Transm Dis AIDS 2019; 40(1):46-50. doi: 10.4103/ijstd.IJSTD_81_17 [Crossref] [ Google Scholar]
- Surti SB, Kosambiya JK, Khokhar N, Patni MM, Gohil AH, Kamdar ZN. Rapid response to syphilis outbreak among female sex workers. Indian J Community Med 2017; 42(4):214-7. doi: 10.4103/ijcm.IJCM_254_16 [Crossref] [ Google Scholar]
- Islam S, Das S, Naga D, Taraphdar P. Mental health status and its correlates among people living with HIV/AIDS in a tertiary care center of West Bengal. Int J Res Med Sci 2023; 11(4):1146-52. doi: 10.18203/2320-6012.ijrms20230852 [Crossref] [ Google Scholar]
- UNAIDS. UNAIDS Welcomes Ground-Breaking Decision by India’s Supreme Court That Strikes Down Law Criminalizing LGBTI People. UNAIDS; 2018. Available from: https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2018/september/20180906_India_section377. Accessed May 17, 2025.
- Chakrapani V, Gulfam FR, Arumugam V, Aher A, Shaikh S, Prasad R. Intersectional stigma and gender non-affirmation hinder HIV care engagement among transgender women living with HIV in India. AIDS Care 2023; 35(4):572-80. doi: 10.1080/09540121.2022.2099511 [Crossref] [ Google Scholar]
- Azhar S, Jokhakar V, Vaudrey J, Gandham S, Oruganti G, Yeldandi V. Associations between HIV stigma, gender, and depression among people living with HIV in Hyderabad, India. J Community Psychol 2023; 51(3):1060-77. doi: 10.1002/jcop.22934 [Crossref] [ Google Scholar]
- UNAIDS. HIV and Transgender and Other Gender-Diverse People. Geneva: UNAIDS; 2019. Available from: https://www.unaids.org/sites/default/files/media_asset/04-hiv-human-rights-factsheet-transgender-gender-diverse_en.pdf.
- Heylen E, Chandy S, Shamsundar R, Nair S, Ravi Kumar BN, Ekstrand ML. Correlates of and barriers to ART adherence among adherence-challenged people living with HIV in southern India. AIDS Care 2021; 33(4):486-93. doi: 10.1080/09540121.2020.1742862 [Crossref] [ Google Scholar]
- Joglekar N, Paranjape R, Jain R, Rahane G, Potdar R, Reddy KS. Barriers to ART adherence & follow ups among patients attending ART centres in Maharashtra, India. Indian J Med Res 2011; 134(6):954-9. doi: 10.4103/0971-5916.92642 [Crossref] [ Google Scholar]