J Educ Community Health. 12(1):1-10.
doi: 10.34172/jech.3204
Original Article
Effects of Health Education and Nutrient Intake Interventions on the Prevention of Treatment Failure Among Patients With Active Tuberculosis in Kericho County, Kenya
Kirui Collins Kipkosgei Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Writing – original draft, 1, 2, * 
George Makalliwa Resources, Supervision, Validation, Visualization, 1
Calvince Otieno Anino Formal analysis, Software, Writing – review & editing, 2
Author information:
1Department of Environment and Disease Control, School of Public Health, Jomo Kenyatta University of Agriculture and Technology, JKUAT, Kenya
2Department of Public Health, School of Health Science, University of Kabianga, Kericho, Kenya
Abstract
Background: Treatment failure remains a significant challenge in the prevention and control of tuberculosis (TB) globally. Despite implemented strategies, TB remains a major cause of death worldwide. This study aimed to determine the effect of health education and nutrient intake intervention on treatment outcomes among patients with active TB.
Methods: A retrospective study was conducted for positive deviance inquiry in TB treatment sites in both Bureti and Ainamoi sub-counties to assess the predictors of treatment failure among 216 patients who had undergone and completed treatment from June 2022 to December 2022. The findings from the inquiry were used to design an intervention on health education and nutrient intake. This quasi-experimental study included 192 patients with smear-positive sputum results at diagnosis, with each group having an equal number of participants.
Results: Treatment success for the control and intervention groups was 77.2% and 93.5%, respectively. Negative medication experience had an increased likelihood of treatment failure (adjusted odds ratio [AOR]=3.080, 95% confidence interval [CI]: 1.139–10.844, P=<0.001). Not having a treatment adherence supporter had significantly higher odds of treatment failure (AOR=1.396, 95% CI: 1.053-1.825, P=0.033). After the intervention, the group that received health education and consumed nutrient-dense meals displayed significantly higher energy intake, protein intake, and fat intake (P<0.01) compared to the control group.
Conclusion: Overall, health education and nutrient intake interventions had a positive influence on the treatment outcome of patients with active TB.
Keywords: Tuberculosis, Treatment failure, Nutrient intake
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Kipkosgei KC, Makalliwa G, Anino CO. Effects of health education and nutrient intake interventions on the prevention of treatment failure among patients with active tuberculosis in Kericho County, Kenya. J Educ Community Health. 2025; 12(1):1-10. doi:10.34172/jech.3204
Introduction
Tuberculosis (TB) is one of the top ten causes of death in the world and is also a major concern for public health (1). An estimated 10.6 million new cases of TB were recorded in 2021, and 1.6 million people died from the disease (2–4). TB continues to be a major public health concern in Kenya, with the country being in the top 10 of the world’s high-burden TB nations (4). For instance, Kenya reported a prevalence rate of 194 cases per 100 000 population in 2022 and a nearly similar prevalence, that is, 197 cases per 100 000 population, in 2023. On average, globally, 1.7% of patients with active TB developed treatment failure (5), whereas in Kenya, the incidence of treatment failure was 3.5% in 2021 (6). Treatment failure is defined as having positive sputum test results at five months of anti-TB treatment after the initiation of treatment (7).
Despite various interventions aimed at reducing treatment failure, such as directly observed therapy, patient education initiatives, and community health strategies, the rates of treatment failure remain alarmingly high. In Kenya, recent data indicate that the treatment success rate stands at 77%, which is short of the target of 80% (8-10). Treatment failure is exacerbated by several factors, including non-adherence to medication, drug-resistant TB, comorbidities and extreme biological variation, low level of health education for the patient, undernutrition, and lack of knowledge related to the disease (11,12). Additionally, alcohol and tobacco use, undernutrition, and poor nutrient intake are other factors associated with treatment failure among patients with active TB (8-9,13).
In Kericho county, where the current study was set, the situation mirrors national trends. The region has reported significant challenges related to TB treatment adherence and success rates. Local health facilities have noted that many patients discontinue their treatment prematurely, often due to a lack of understanding about the importance of completing their regimen and adhering to the prescription (6). Moreover, comorbidities such as HIV and lifestyle factors, such as alcohol and tobacco use, that are prevalent in the area further complicate treatment outcomes.
The current research aims to assess the impact of health education and nutritional interventions on TB treatment failure among patients with active TB in Kericho county. While similar studies have been conducted previously, this research was motivated by the need to explore the specific roles that health education and nutritional status played in enhancing treatment adherence and success. The integration of these variables was crucial because previous interventions had predominantly focused on medication adherence while failing to adequately address the nutritional needs, which is a significant gap identified by the World Health Organization as a contributing factor to treatment failure.
The importance of this current study lies not only in its potential to improve individual patient outcomes but also in its broader implications for public health strategies aimed at controlling TB transmission in Kenya by adopting practices that have previously worked among those who successfully completed their treatments. By identifying effective interventions that simultaneously enhance patient education and nutritional intake, this study can inform policies that lead to more comprehensive approaches for managing TB treatment failures (14,15). Ultimately, addressing these gaps can significantly reduce the burden of TB in economically productive populations, thereby improving overall public health and economic stability in the region.
Materials and Methods
Study Design and Area
A hybrid study design comprising both retrospective and prospective study components was used in this study (16,17). The retrospective study was designed as a cross-sectional study, whereas the prospective component was designed as a pre-post quasi-experiment with both intervention and control study groups. The study was conducted in two different study sites, Bureti and Ainamoi sub-counties, which are both located in Kericho, Kenya (Figure 1).
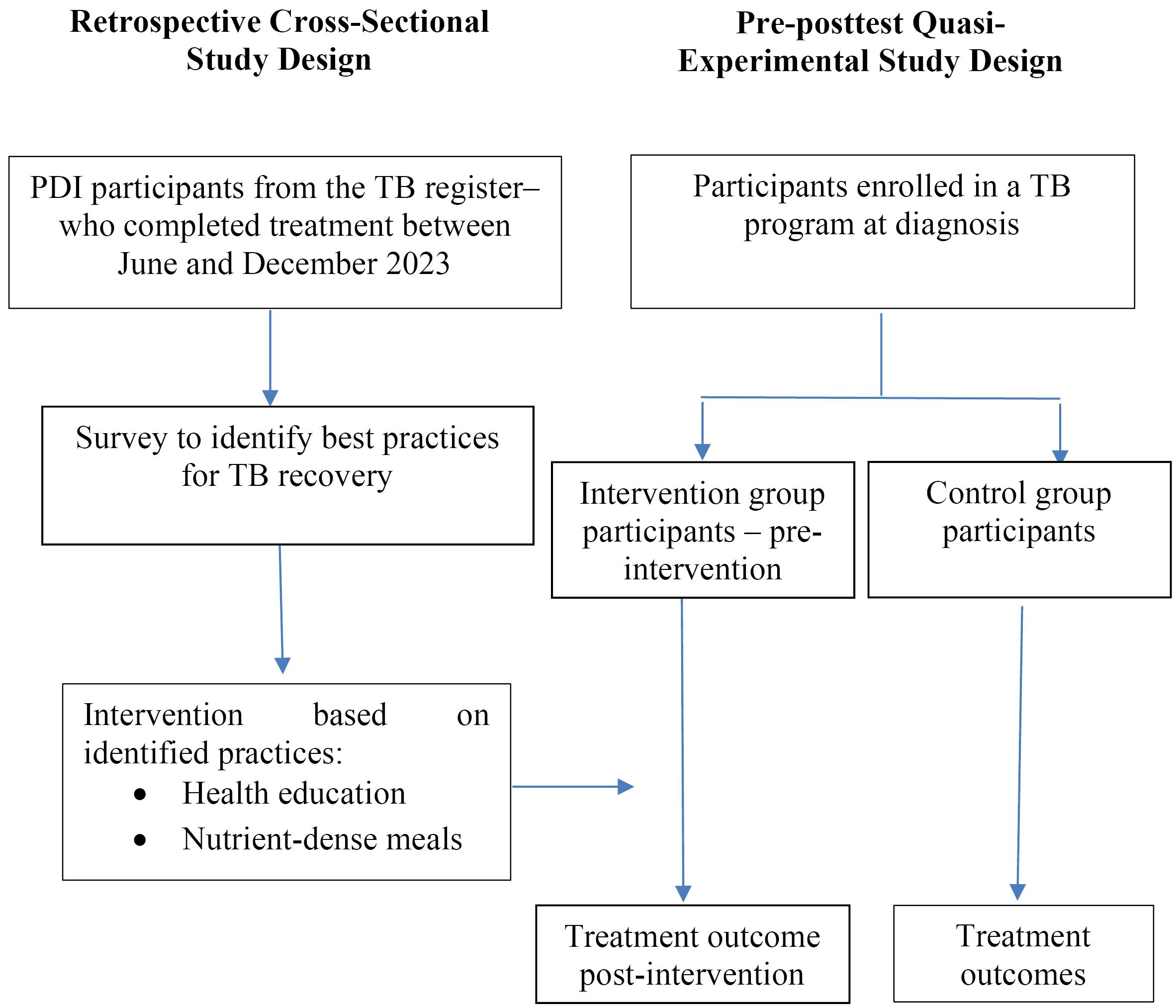
Figure 1.
Flowchart of the Study Design and Execution Processes. Note. PDI: Positive deviance inquiry; TB: Tuberculosis
.
Flowchart of the Study Design and Execution Processes. Note. PDI: Positive deviance inquiry; TB: Tuberculosis
Sampling Strategy
The study was performed at two levels in tandem with previous studies based on the positive deviance model (15,17). The first level was positive deviance inquiry (PDI), an approach that was retrospectively conducted to identify the ‘best practices’ that promoted recovery from TB, while the second level was an intervention based on the identified ‘best practices. The participants for PDI were selected from the TB register using systematic random sampling. The inclusion criterion for these participants was the completion of TB treatment. Overall, 216 participants were included in the first level of the study as determined using the Fischer formula. At the second level, multistage cluster sampling was adopted for both intervention and control study groups. It was used to identify and recruit participants for the study. At the onset, Bureti and Ainamoi sub-counties were purposively sampled as the intervention and control study sites, respectively, which formed the first stage. These two sub-counties were specifically chosen due to their high proportion of treatment failures, 5.7% and 4.3%, respectively (6,18). In the second stage, the investigators adopted the simple random sampling technique to select 8 out of the 13 health facilities that were utilized as TB treatment sites for patients with TB disease at the time of study in both the Ainamoi and Bureti sub-counties. In the last stage, 11 groups of 18 patients were recruited at diagnosis, totaling 198 participants for both intervention and control groups. At first diagnosis, all patients who met the inclusion criteria were recruited in the study. However, six of the sampled participants were excluded from the study based on the established exclusion criteria. The inclusion criteria adopted in the current study included being smear positive for sputum TB results, diagnosed within a month prior to the onset of the study, and registered as an active TB case in the study sites. On the other hand, those who had life-threatening complications or were hospitalized or pregnant at the time of the study were excluded from the investigation (19). The sampled participants were equally distributed to the two study groups.
Study Tools and Data Collection
Positive Deviance Inquiry
A researcher-administered questionnaire was used to collect information on the practices of the respondents who took part in the PDI in February 2023. The data gathered on practices were associated with sociodemographic characteristics, dietary intake at the time of their medication, and health-seeking behaviors. Additionally, their retrospective data on nutritional status and sputum results were retrieved from the medical records at their respective treatment sites. Moreover, information on their treatment outcome upon completion of the treatment regimen was obtained from the records. The PDI questionnaire was administered to the respondents prior to the onset of the intervention at their place of residence. The questionnaire was designed to assess various sociodemographic, clinical, and behavioral factors related to TB treatment and patient outcomes. Key variables included demographic information (age, gender, education, occupation, and income), health status (body mass index [BMI], sputum results, and comorbidities), healthcare access (clinic accessibility, waiting times, and drug availability), adherence (drug intake, side effects, and treatment completion), and knowledge and attitudes toward TB. The estimated time to administer the questionnaire was approximately 30 minutes.
Intervention and Control Groups
The data were collected from March 2023 to September 2023 for both control and intervention groups. Positive deviance practices identified through the PDI process, together with nutrient-dense meals, formed the study interventions, which were delivered as two packages (health education and a nutrient-dense meal). Each of the positive deviance intervention groups was taken through two hours of health education sessions held in an outdoor location, followed by a nutrient-dense meal prepared at the intervention site. This was performed every fortnight for 6 months. The health education messages were on a health education protocol containing the positive deviance practices identified from the PDI. They included adherence to medication, identification and acceptance of treatment supporters, alcohol and tobacco use and its implications during medication, adequate house ventilation, a balanced diet, and food preparation.
A questionnaire aligned with this protocol was employed to assess the attainment of the health education outcomes. A similar questionnaire was utilized for the control group. It was designed to assess sociodemographic traits, adherence to medication, identification and acceptance of treatment supporters, alcohol and tobacco use and its implications during medication, and adequate house ventilation. Key variables were demographic information (age, gender, education, occupation, and income), health status (BMI, sputum results, and comorbidities), healthcare access (clinic accessibility, waiting times, and drug availability), and adherence (drug intake, side effects, and treatment completion). The other variables included treatment supporter (sharing of the TB status, reminder to take medication, and the person informed), financial supporter (the provider of the needed support), and adequate house ventilation (the household size, number of windows and doors, number of permanent vents, and room space). Approximately 30 minutes were allocated to questionnaire administration.
Additionally, dietary history was self-reported using a 7-day standard food frequency questionnaire, which was administered to both groups. In addition to the food frequency questionnaire, the other questionnaires used in the study were subjected to a panel of six experts in the Department of Public Health at the host University for validation purposes. This was followed by piloting to refine the participant’s feedback. The reliability of the questionnaires was tested using Cronbach alpha tests, and correlation scores of 0.89 and 0.83 were obtained for the PDI questionnaire and health education outcomes questionnaire, respectively. The questionnaires were administered on the day of their recruitment into the study and six months later. These questionnaires were administered at the TB treatment sites, where the participants were enrolled for their medication. All the questionnaires were research administered.
Data Analysis
The collected data were analyzed using the Statistical Package for Social Sciences (SPSS), version 23. The normal distribution of the data for nutrient intake was assessed using the Kolmogorov-Smirnov test (P = 0.27). Descriptive analyses were conducted to summarize sociodemographic characteristics and TB treatment outcomes. BMI was scored based on underweight, normal, and overweight categories according to the WHO BMI categorization indicator (5). Chi-square tests were utilized to explore associations between sociodemographic factors and treatment failure. Further, binary logistic regression was employed to identify key factors associated with treatment failure. This was accomplished by initially identifying the significant predictors through univariable analysis, which were then included in the final model. Adjusted odds ratios (AOR) and 95% confidence intervals (CIs) were calculated to assess the strength of these associations. Moreover, nutrient intake values, including energy, protein, fat, carbohydrates, vitamins, and minerals, were compared at baseline and endline for both groups using means and standard deviations. Furthermore, nutrient intake changes between control and intervention groups at baseline and endline were analyzed using a two-tailed independent t-test. The significance was set at P ≤ 0.05 for all statistical tests.
Results
Response Rate
The baseline response rate was 94% (n = 192). Endline response rate was 91.7% (n = 88) and 97.9% (n = 94) in the control and intervention groups, respectively. The variation between baseline and endline data was a result of the participant’s loss to follow up for those in the intervention and both loss to follow up and attrition for those in the control group.
Sociodemographic Characteristics of Participants During Positive Deviance Inquiry
The age distribution showed that the majority of respondents (58.8%) were within the 18–35 age range, followed by 34.3% in the 36–59 age group. A significant majority of the respondents were Christians (81.9%) compared to non-Christians (18.1%). In terms of gender, 67.6% of respondents were male, while 32.4% were female. As regards marital status, 41.2% were married. Additionally, the majority of the respondents had a primary level of education (40.6%) and were self-employed (48.6%). Regarding housing, the majority lived in owned homes (87.5%) and had a monthly income of 82.9% (Table 1).
Table 1.
Demographic and Socio-Economic Characteristics of the Respondents at Positive Deviance Inquiry
|
Variable
|
Frequency (n=216)
|
Percent
|
| Age |
|
|
| 18-35 |
127 |
58.8 |
| 36-59 |
74 |
34.3 |
| ≥ 60 |
15 |
6.9 |
| Religion |
|
|
| Christian |
177 |
81.9 |
| Non-Christian |
39 |
18.1 |
| Gender |
|
|
| Male |
146 |
67.6 |
| Female |
70 |
32.4 |
| Marital status |
|
|
| Married |
89 |
41.2 |
| Single |
93 |
43.1 |
| Separated |
14 |
6.5 |
| Window/widower |
10 |
4.6 |
| Divorced |
10 |
4.6 |
| Education |
|
|
| Informal education |
16 |
7.3 |
| Primary |
88 |
40.6 |
| Secondary |
83 |
38.5 |
| Tertiary |
29 |
13.6 |
| Occupation |
|
|
| Formal employment |
19 |
8.8 |
| Self-employment |
105 |
48.6 |
| Unemployed |
92 |
42.6 |
| Adequate ventilation |
|
|
| Yes |
189 |
87.5 |
| No |
27 |
12.5 |
| Average monthly income |
|
|
| < 5000 Ksh. |
159 |
74 |
| 5001-10000 Ksh. |
34 |
15.6 |
| 10001-15000 Ksh. |
13 |
5.8 |
| > 15001 Ksh. |
10 |
4.6 |
Characteristics of Participants in the Intervention and Control Groups at Baseline and Endline
A total of 192 respondents were recruited and divided into control (n = 96) and intervention groups (n = 96). However, attrition occurred during the study, reducing the number of respondents to 88 in the control group and 94 in the intervention group. There were no significant differences regarding the sociodemographic and economic characteristics of the respondents between the intervention and control groups at baseline and end-line (Table 2).
Table 2.
Demographics and Socioeconomic Characteristics of Participants in the Intervention and Control Groups at Baseline and Endline
|
Variables
|
Baseline
|
χ2
|
P
Value
|
Endline
|
χ2
|
P
Value
|
|
Control
|
Intervention
|
Control
|
Intervention
|
|
n (%)
|
n (%)
|
|
|
n (%)
|
n (%)
|
|
|
| Gender |
|
|
|
|
|
|
|
|
| Female |
31 (32.3) |
30 (31.3) |
0.000 |
1.0 |
30 (34.1) |
30 (31.9) |
1.869 |
0.172 |
| Male |
65 (67.7) |
66 (68.7) |
58 (65.9) |
64 (68.1) |
| Age |
|
|
|
|
|
|
|
|
| 18-35 |
60 (62.5) |
61 (63.5) |
0.954 |
0.621 |
51 (58.0) |
59 (62.8) |
1.437 |
0.488 |
| 36-59 |
29 (30.2) |
28 (29.2) |
28 (31.8) |
27 (28.7) |
| > 60 |
7 (7.3) |
7 (7.3) |
9 (10.2) |
8 (8.5) |
| Marital status |
|
|
|
|
|
|
|
|
| Married |
32 (33.3) |
33 (34.4) |
5.631 |
0.228 |
28 (31.8) |
33 (35.1) |
2.756 |
0.43 |
| Single |
51 (53.1) |
46 (47.9) |
50 (56.8) |
46 (48.9) |
| Separated |
5 (5.2) |
7 (7.3) |
5 (5.7) |
6 (6.4) |
| Widow/widower |
6(6.3) |
5(5.2) |
4(4.6) |
5(5.3) |
| Divorced |
2 (2.1) |
5 (5.2) |
1 (1.1) |
4 (4.3) |
| Education level |
|
|
|
|
|
|
|
|
| No education |
6 (6.3) |
7 (7.3) |
0.233 |
0.974 |
5 (5.7) |
6 (6.4) |
5.773 |
0.123 |
| Primary |
38 (39.6) |
39 (40.6) |
35 (39.8) |
38 (40.4) |
| Secondary |
36 (37.5) |
37 (38.5) |
33 (37.5) |
37 (39.4) |
| Tertiary |
16 (16.6) |
13 (13.6) |
15 (17.0) |
13 (13.8) |
| Employment status |
|
|
|
|
|
|
|
|
| Formal employment |
16 (16.7) |
15 (15.6) |
3.652 |
0.302 |
15 (17.0) |
15 (16.0) |
3.875 |
0.144 |
| Self-employment |
41 (42.7) |
49 (51.1) |
38 (43.2) |
48 (51.1) |
| Unemployed |
39 (40.6) |
32 (33.3) |
35 (39.8) |
31 (32.9) |
| Average monthly income |
|
|
|
|
|
|
|
|
| 0-5000 Ksh. |
76 (79.1) |
72 (75.0) |
4.140 |
0.247 |
72 (81.8) |
70 (74.5) |
3.247 |
0.355 |
| 5001-10000 |
7 (7.3) |
14 (14.6) |
6 (6.8) |
14 (14.9) |
| 10001-15000 |
6 (6.3) |
6 (6.3) |
5 (5.7) |
6 (6.3) |
| > 15001 |
7 (7.3) |
4 (4.1) |
5 (5.7) |
4 (4.3) |
| Employment status |
|
|
|
|
|
|
|
|
| Formal employment |
16 (16.7) |
15 (15.6) |
3.652 |
0.302 |
15 (17.0) |
15 (16.0) |
3.875 |
0.144 |
| Self-employment |
41 (42.7) |
49 (51.1) |
38 (43.2) |
48 (51.1) |
| Unemployed |
39 (40.6) |
32 (33.3) |
35 (39.8) |
31 (32.9) |
Treatment Outcomes Among Respondents in the Intervention and Control Groups
The prevalence of treatment failure in the control group was high (15.7%), which greatly contributed to the high proportion, that is, 3.0% of deaths within the group. The majority of TB patients in the intervention group (90.3%) were cured compared to the 70% in the control group. Treatment completion rate and losses to follow up were high in the control group (6.0% and 4.1%, respectively, Figure 2).
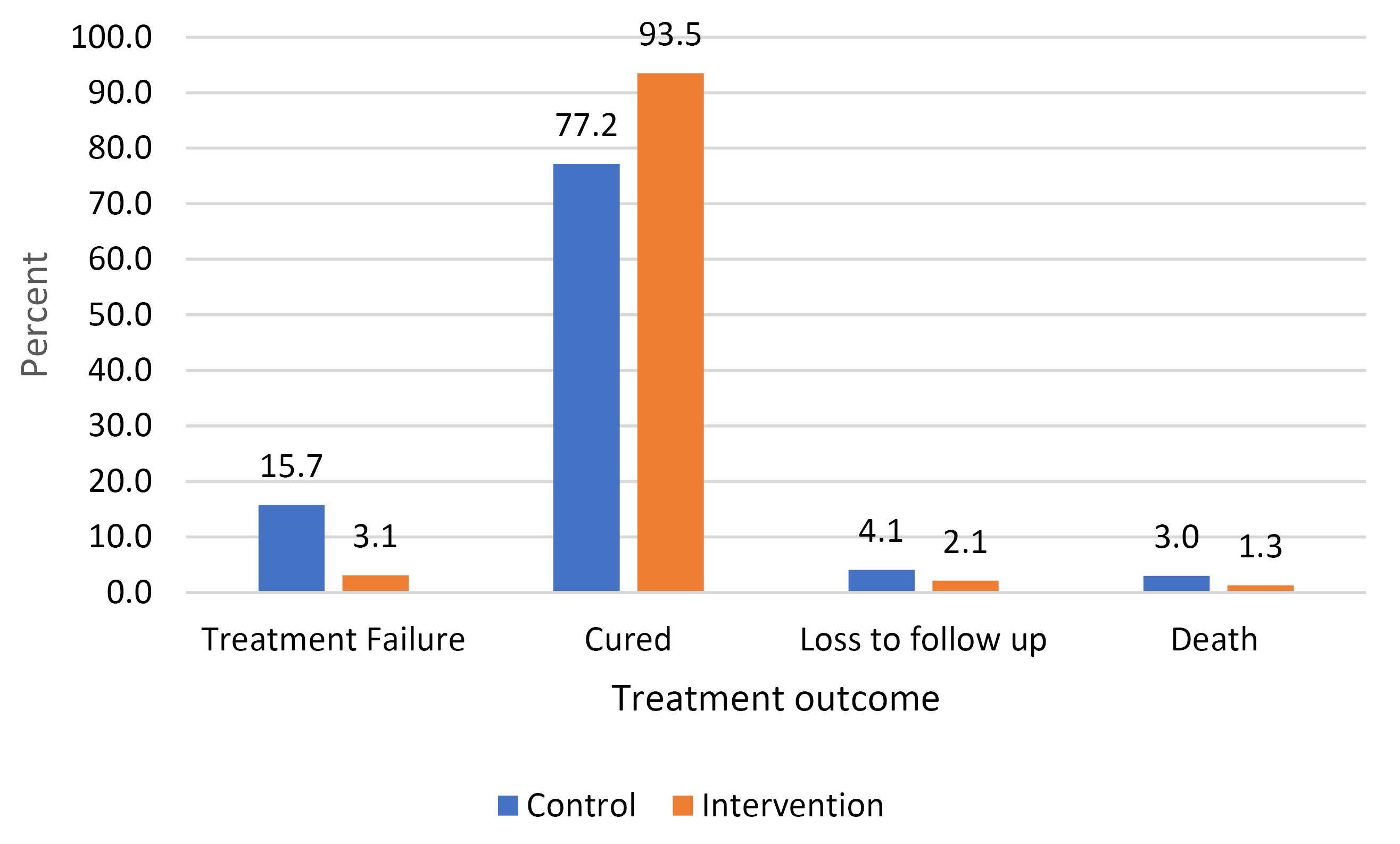
Figure 2.
Prevalence of TB Treatment Outcome for the Control and Intervention Groups. Note. TB: Tuberculosis
.
Prevalence of TB Treatment Outcome for the Control and Intervention Groups. Note. TB: Tuberculosis
Factors and Practices Associated With Treatment Failure
While adjusting for age and gender, our results demonstrated a significant association between treatment failure and some predictor variables, such as religion, BMI, TB medication experience, financial treatment support, treatment adherence supporter, and presence of comorbidities (Table 3). The findings revealed that participants who were non-Christians had significantly lower odds of experiencing treatment failure compared to Christians (AOR = 0.118, 95% CI: 0.0345-0.404, P ≤ 0.001). Similarly, those who were overweight at the endline were three times more likely to develop treatment failure in comparison to their underweight counterparts (AOR = 3.515, 95% CI: 1.139-10.844, P = 0.029). Patients with negative TB medication experiences had a higher chance of treatment failure compared to those with positive TB medication experiences (AOR = 3.080, 95% CI: 1.139-10.844, P ≤ 0.001). Additionally, individuals without treatment adherence supporters and those who failed to adhere to medication had significantly higher odds of developing treatment failure in comparison to their counterparts (AOR = 1.396, 95% CI: 1.053-1.825, P = 0.033 and AOR = 2.034, 95% CI: 1.002-7.488, P = 0.013, respectively). On the other hand, participants without comorbidities were less likely to develop treatment failure (AOR = 0.07, 95% CI: 0.010-0.495, P = 0.008). Healthcare-related factors comprising poor staff attitude and delayed opening of the TB clinic significantly increased the chances of developing treatment failure (AOR = 0.059, 95% CI: 0.006-0.599, P = 0.017).
Table 3.
Multivariate Analysis of Predictors of Treatment Failure Among the Respondents
|
Variable
|
AOR
|
95% CI
|
P
Value
|
| Religion |
|
|
|
| Christian |
Ref. |
|
|
| Non-Christian |
0.118 |
0.034-0.404 |
< 0.001 |
| Adequate ventilation |
|
|
|
| Yes |
Ref. |
|
|
| No |
0.312 |
0.090-1.080 |
0.066 |
| BMI at the end |
|
|
|
| Underweight |
|
|
Ref. |
| Normal |
0.372 |
0.020-6.832 |
0.506 |
| Overweight |
3.515 |
1.139-10.844 |
0.029 |
| TB medication experience |
|
|
|
| Positive |
Ref. |
|
|
| Negative |
3.080 |
1.609-5.895 |
< 0.001 |
| Treatment adherence supporter |
|
|
|
| Household member |
|
|
Ref. |
| Non-household member |
1.204 |
0.740-1.646 |
0.631 |
| No supporter |
1.396 |
1.053-1.825 |
0.033 |
| Tobacco and alcohol use |
|
|
|
| Yes |
|
|
Ref. |
| No |
2.883 |
0.295-28.170 |
0.363 |
| Presence of comorbidities |
|
|
|
| Yes |
|
|
Ref. |
| No |
0.070 |
0.010-0.495 |
0.008 |
| Adherence to medication |
|
|
|
| Yes |
|
|
Ref. |
| No |
2.034 |
1.002-7.488 |
0.013 |
| Healthcare-related factors |
|
|
|
| Yes |
Ref. |
|
|
| No |
0.059 |
0.006-0.599 |
0.017 |
Note. AOR: Adjusted odds ratio; CI: Confidence interval; BMI: Body mass index; TB: Tuberculosis.
Nutrient Intake of Participants
The BMI was not statistically different in the intervention and control groups at baseline and endline (Table 4). At baseline, energy, protein, and fat intake were comparable between the control and intervention groups. After the intervention, the group that received health education and consumed nutrient-dense meals displayed significantly higher energy intake (P = 0.001), protein intake (P < 0.001), and fat intake (P < 0.0001) compared to the control group. Although carbon and fibre consumption did not differ significantly at baseline, the intervention group consumed both of them notably more at the endline assessment (P < 0.001). Baseline vitamin A-RAE and vitamin C intake were comparable between the control and intervention groups. A marked improvement in the consumption of both vitamins was evident in the intervention group post-intervention, while the control group showed no such change (P < 0.001). A similar trend was observed with regard to the intake of minerals, such as zinc (P < 0.001) and selenium (P < 0.001).
Table 4.
Nutrient Intake of Participants at Baseline and Endline for the Intervention and Control Groups
|
Variable
|
Baseline
|
P
Value
|
Endline
|
P
Value
|
|
Control
|
Intervention
|
Control
|
Intervention
|
| BMI |
20.94 ± 3.01 |
18.25 ± 2.9 |
0.163 |
20.08 ± 3.10 |
20.76 ± 3.46 |
0.264 |
| Energy (kcal) |
1476.57 ± 745.14 |
1410.82 ± 656.77 |
0.510 |
1347.06 ± 477.80 |
2072.62 ± 680.59 |
< 0.001 |
| Protein (g) |
96.42 ± 67.10 |
81.79 ± 47.76 |
0.074 |
87.52 ± 24.36 |
97.60 ± 52.70 |
< 0.001 |
| Fat (g) |
45.99 ± 34.17 |
45.88 ± 21.86 |
0.078 |
43.61 ± 13.32 |
82.89 ± 23.37 |
< 0.001 |
| Cabohydrate (g) |
149.37 ± 86.53 |
156.63 ± 50.57 |
0.101 |
146.23 ± 40.25 |
221.05 ± 56.86 |
< 0.001 |
| Fibre (g) |
39.03 ± 21.80 |
22.11 ± 10.29 |
0.098 |
9.92 ± 8.13 |
26.12 ± 12.43 |
< 0.001 |
| Vitamin A-RAE (mcg) |
1049.49 ± 690.81 |
674.11 ± 402.19 |
0.074 |
592.97 ± 209.44 |
809.09 ± 397.78 |
< 0.001 |
| Vitamin C (mg) |
171.33 ± 117.99 |
98.97 ± 62.64 |
0.231 |
32.55 ± 35.29 |
115.61 ± 63.72 |
< 0.001 |
| Zinc (mg) |
11.72 ± 10.72 |
8.08 ± 5.52 |
0.129 |
4.00 ± 4.19 |
9.32 ± 5.26 |
< 0.001 |
| Selenium (mcg) |
58.05 ± 54.30 |
48.82 ± 32.31 |
0.142 |
19.31 ± 20.99 |
31.15 ± 3.11 |
< 0.001 |
Note. BMI: Body mass index.
Discussion
Nearly similar treatment failure rates were found among our study participants in the control group and those reported in the literature, which ranged from 5.4% to 15.7% in some areas in Kenya (6). In our study, slightly lower rates of treatment failure were observed among participants in the intervention group compared to earlier studies within similar settings to our study that reported treatment failure rates of 3.8–4.4 (8). The difference in our observations could be due to variances in the nature of the interventions. The earlier studies adopted a single intervention strategy, whereas our study utilized a multiple-intervention approach comprising both health education and nutrient intake. Additionally, as reported in previous research (12), differences in outcomes among participants regarding the intervention could be beyond the specifics of the intervention, including factors such as race, religion, gender, level of education, source of income, and level of income. Indeed, our results confirmed an association between religious beliefs and treatment outcomes for TB patients. Individuals who identified as Christian had lower rates of treatment failure, which conforms to the findings of previous studies, showing improved treatment outcomes among TB patients who ascribed to a religious community (20-24). An earlier study indicated that the role of religious communities in providing consistent social support networks can persuade adherence to treatment plans and enhance the overall well-being of patients by offering a sense of hope (24-26). However, other studies reported the negative effects of religious beliefs that led to patients abandoning medical treatment (27,28).
The demanding nature of the TB treatment regimen involves several drugs taken simultaneously for at least six months or more. The utilization of drugs for long periods can be challenging for patients. Our results demonstrated the critical role of good adherence in achieving positive TB treatment outcomes. Our findings are in line with earlier reports, indicating an association among adherence, treatment adherence supporter, and treatment outcome (29). However, our study delved deeper into the nature of this association with regard to the occurrence of treatment failure among TB patients who adhered to medication and had adherence treatment supporters. Existing information showed that good adherence to TB medication led to a positive outcome (29,30). At the same time, the same study reported that the consequences of non-adherence to TB therapy increased the transmission, morbidity, emergence of treatment failure, drug-resistant TB, and mortalities. Some of the factors earlier reported to contribute to non-adherence are limited patient knowledge, financial difficulties, and adverse drug reactions (31,32). Some studies demonstrated that health education on the benefits of adherence, the need for treatment adherence supporters, and the consequences of non-adherence were crucial components of TB care that could play a critical role in addressing challenges leading to non-adherence and thereby improving treatment response (12,13). The intervention in the current study had similar components that could potentially explain our satisfactory outcomes. Our findings revealed a direct positive association between adherence to treatment supporter and non-occurrence of treatment failure, which corroborates the results of earlier studies (12,13,29,30). However, unlike the earlier studies that demonstrated that having support from family members was strongly associated with lower rates of treatment failure, the results of our study confirmed that regardless of the supporter’s relationship, their involvement significantly reduced the likelihood of treatment failure. Our results are in conformity with those of studies by Chen et al, reporting that having a companion during medication could play an important role in encouraging, supporting, and supervising the patient’s medication (33), and Mariani et al, demonstrating the need for intentional support for patients on TB treatment (34). Our findings further emphasized the importance of medication experience in achieving successful TB treatment outcomes and minimizing treatment failure. A positive correlation between medication experience and treatment outcome was reported in previous studies (27,29). Regarding comorbidities, our study found that patients with other conditions experienced poor treatment outcomes, an observation that is in agreement with the results of earlier studies, indicating that the presence of underlying disease was associated with TB treatment failure (30,32). Other studies reported that HIV co-infection significantly affected the overall TB treatment success rate and TB-related mortalities (32,33). It is, therefore, imperative to understand the health status of TB patients for proper support. In terms of healthcare-related factors, which often vary, positive results were observed in treatment outcomes in our study. The findings of other studies are in agreement with those of our study, representing that healthcare-related factors positively contribute to the realization of positive outcomes (31,35). In our study, this improvement could be attributed to the presence of skilled staff, the use of proper health equipment, and the timely opening of the TB clinics.
In our study, a significant improvement was found in nutrient intake among TB patients at the endline in the intervention group. This enhanced nutrient intake improved BMI from the low levels recorded at baseline to the normal range at the endline. The improved BMI status and other important nutrients in turn addressed undernutrition, which is associated with poor treatment outcomes among patients with TB (36). Endline BMI proved to be a crucial factor in determining treatment outcomes, with overweight individuals exhibiting increased susceptibility to treatment failure. This is a unique finding contrary to the existing evidence, where overweight has been noted to have beneficial effects (26–28). Even though in our study, the majority of those who were overweight had poor medication adherence, a factor that is reported to result in poor treatment outcomes (35,36), this discrepancy requires further study to understand the cause of the anomaly. The increased energy, protein, fibre, and fat intake observed in the intervention group at the study conclusion affirms the importance of nutritional therapy for patients with active TB. Another research confirmed that active TB, similar to other infectious diseases, can increase energy, protein, fibre, and fat requirements by the body (36), thus explaining the diminished intake of the macronutrients by the control group at the endline compared to the baseline assessment. The findings conform to those of previous studies, indicating that nutritional therapy potentially contributes to positive health outcomes in various human pathologies (28,37-38). Our finding revealed significant improvements in micronutrient intake, particularly zinc, selenium, vitamin A, and vitamin C, among the intervention group at endline assessment. This is attributed to the nutrition intervention and is in concurrence with previous studies, demonstrating that micronutrient demand for active TB patients increased during the first 4 months of treatment, which is an indication that patients needed food supplementation or rations for positive treatment outcomes (39,40). Based on our findings, nutritional intervention is an essential component in active TB treatment for the realization of positive treatment outcomes.
Our findings should be interpreted with caution since we used a quasi-experimental design rather than a randomized controlled trial. Our choice of study design may have introduced selection bias, which could affect the generalizability of the findings. Additionally, the study did not account for seasonal variations in food availability and affordability, which could have influenced the participants’ ability to maintain the recommended nutrient intake levels.
Conclusion
Our findings revealed that the combination of health education and nutrient intake is a good strategy for improving TB treatment outcomes. This approach addressed the common challenges observed among TB patients on medication, including low BMI, undernutrition, non-adherence to medication, negative medical experience, lack of adherence to treatment supporter, presence of comorbidities, and poor attitudes with regard to healthcare services offered at the TB clinic. These findings highlight the importance of a comprehensive approach to TB control through an approach that addresses both the biological and social aspects of the disease. Further research is needed to validate these results in diverse settings and to explore the long-term impact of such interventions. Moreover, future studies should investigate the cost-effectiveness of these interventions to inform resource allocation and policy decisions. By addressing the complex nature of TB and implementing evidence-based interventions, we stand a chance to make significant strides in combating this global health challenge.
Acknowledgements
The authors are grateful for all study participants and everyone from Bureti and Ainamoi sub-counties who had an inseparable input to the success of this study.
Competing Interests
The authors declared no potential conflict of interests with respect to research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review and Ethics Committee of the University of Eastern Africa, Baraton (IREC No. B0207122022), and subsequently approved by Kericho County Referral Hospital. Additionally, a research permit was obtained from the National Commission of Science and Technology (NACOSTI/P/23/23219), and further permission was sought from the Kericho County Commissioner Office (MISC.19 VOL.III/68) and the Kericho County Education Office (KER/C/ED/GC/2/VOL.II 1/16). Patients’ consent was sought both verbally and in writing. Further, the researcher ensured the privacy and confidentiality of the respondent’s participation and information. Each respondent was given a unique identification code, which was known only to the investigator. Moreover, the collected data were hosted on a central server, which could only be accessed by the researcher.
Funding
None.
References
- Singh AK, Siddhanta A, Goswami L. Improving tuberculosis treatment success rate through nutrition supplements and counselling: findings from a pilot intervention in India. Clin Epidemiol Glob Health 2021; 11:100782. doi: 10.1016/j.cegh.2021.100782 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Tuberculosis Report. Geneva, Switzerland: WHO; 2022.
- Litvinjenko S, Magwood O, Wu S, Wei X. Burden of tuberculosis among vulnerable populations worldwide: an overview of systematic reviews. Lancet Infect Dis 2023; 23(12):1395-407. doi: 10.1016/s1473-3099(23)00372-9 [Crossref] [ Google Scholar]
- Tayal A, Kabra SK. Tuberculosis preventive treatment. Indian J Pediatr 2024; 91(8):823-9. doi: 10.1007/s12098-023-04969-z [Crossref] [ Google Scholar]
- World Health Organization (WHO). Global Tuberculosis Report. Geneva, Switzerland: WHO; 2020.
- Ministry of Health. National Tuberculosis, Leprosy and Lung Disease Program. Nairobi, Kenya: Ministry of Health; 2021.
- Ministry of Health. Guidelines on the Programmatic Management of Drug Resistant Tuberculosis 2020. Nairobi, Kenya: Ministry of Health; 2021.
- Alipanah N, Jarlsberg L, Miller C, Linh NN, Falzon D, Jaramillo E. Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies. PLoS Med 2018; 15(7):e1002595. doi: 10.1371/journal.pmed.1002595 [Crossref] [ Google Scholar]
- Kipkosgei KC, Anino CO, Makalliwa G. Effects of positive deviance nutrition intervention on sputum smear conversion among patients on tuberculosis medication in Kericho county, Kenya. Indian J Tuberc 2025; 72 Suppl 1:S68-74. doi: 10.1016/j.ijtb.2025.02.006 [Crossref] [ Google Scholar]
- de Faria Gomes NM, da Mota Bastos MC, Marins RM, Barbosa AA, Soares LC, de Oliveira Wilken de Abreu AM. Differences between risk factors associated with tuberculosis treatment abandonment and mortality. Pulm Med 2015; 2015:546106. doi: 10.1155/2015/546106 [Crossref] [ Google Scholar]
- Diallo A, Dahourou DL, Dah TTE, Tassembedo S, Sawadogo R, Meda N. Factors associated with tuberculosis treatment failure in the Central East Health region of Burkina Faso. Pan Afr Med J 2018; 30:293. doi: 10.11604/pamj.2018.30.293.15074 [Crossref] [ Google Scholar]
- Sawadogo B, Tint KS, Tshimanga M, Kuonza L, Ouedraogo L. Risk factors for tuberculosis treatment failure among pulmonary tuberculosis patients in four health regions of Burkina Faso, 2009: case control study. Pan Afr Med J 2015; 21:152. doi: 10.11604/pamj.2015.21.152.4827 [Crossref] [ Google Scholar]
- Vasankari T, Holmström P, Ollgren J, Liippo K, Kokki M, Ruutu P. Risk factors for poor tuberculosis treatment outcome in Finland: a cohort study. BMC Public Health 2007; 7:291. doi: 10.1186/1471-2458-7-291 [Crossref] [ Google Scholar]
- Asres A, Jerene D, Deressa W. Delays to treatment initiation is associated with tuberculosis treatment outcomes among patients on directly observed treatment short course in Southwest Ethiopia: a follow-up study. BMC Pulm Med 2018; 18(1):64. doi: 10.1186/s12890-018-0628-2 [Crossref] [ Google Scholar]
- Anino CO, Were GM, Khamasi JW. Positive deviant intervention prevents acute malnutrition in younger siblings of undernourished children in Migori county, Kenya. J Nutr Diet 2018; 2(1):21-7. [ Google Scholar]
- Anino CO, Mibei EK, Kipkosgei KC, Wanzala J. The role of health education in COVID-19 vaccine hesitancy among outpatients in Kericho county, Kenya An Institution Based Cross Sectional Survey. International Journal of Multidisciplinary Research and Innovation 2024; 2(2):15-21. [ Google Scholar]
- Anino OC, Were GM, Khamasi JW. Impact evaluation of positive deviance hearth in Migori county, Kenya. Afr J Food Agric Nutr Dev 2015; 15(5):10578-96. doi: 10.18697/ajfand.72.15395 [Crossref] [ Google Scholar]
- Ministry of Health. Kericho TB Cases by Sub-County. Kericho, Kenya: Ministry of Health; 2019.
- Calderwood CJ, Wilson JP, Fielding KL. Dynamics of sputum conversion during effective tuberculosis treatment: A systematic review and meta-analysis. PLoS Med 2021; 18(4):e1003566. doi: 10.1371/journal.pmed.1003566 [Crossref] [ Google Scholar]
- John S, Abdulkarim S, Martins OF. Assessment of knowledge, attitude, and practices on tuberculosis amongst nomads in Adamawa state, Nigeria. Texila Int J Public Health 2024; 12:1-16. doi: 10.21522/TIJPH.2013.12.01.Art028 [Crossref] [ Google Scholar]
- Heukelbach J, de Oliveira FA, Hesse G, Feldmeier H. Tungiasis: a neglected health problem of poor communities. Trop Med Int Health 2001; 6(4):267-72. doi: 10.1046/j.1365-3156.2001.00716.x [Crossref] [ Google Scholar]
- Manurung N. Involving religious organizations in improving TB medication adherence. Indian J Tuberc 2024; 71 Suppl 2:S191-6. doi: 10.1016/j.ijtb.2023.04.017 [Crossref] [ Google Scholar]
- Machmud R, Medison I, Yani FF. Cultural and religious belief approaches of a tuberculosis program for hard-to-reach populations in Mentawai and Solok, West Sumatera, Indonesia. Kesmas 2020; 15(4):205-11. doi: 10.21109/kesmas.v15i4.3374 [Crossref] [ Google Scholar]
- Oji VU, Hung LC, Abbasgholizadeh R, Terrell Hamilton F, Essien EJ, Nwulia E. Spiritual care may impact mental health and medication adherence in HIV + populations. HIV AIDS (Auckl) 2017; 9:101-9. doi: 10.2147/hiv.S126309 [Crossref] [ Google Scholar]
- Mobolaji OI. Determinants of tuberculosis services acceptance among patients in Ibadan, Nigeria. Afr J Soc Work 2014; 4(1):82-102. [ Google Scholar]
- Phan MN, Guy ES, Nickson RN, Kao CC. Predictors and patterns of weight gain during treatment for tuberculosis in the United States of America. Int J Infect Dis 2016; 53:1-5. doi: 10.1016/j.ijid.2016.09.006 [Crossref] [ Google Scholar]
- Koo HK, Min J, Kim HW, Lee J, Kim JS, Park JS. Prediction of treatment failure and compliance in patients with tuberculosis. BMC Infect Dis 2020; 20(1):622. doi: 10.1186/s12879-020-05350-7 [Crossref] [ Google Scholar]
- Sarangi MK, Padhi S. An overview of tuberculosis chemotherapy–a literature review. J Appl Pharm Res 2016; 4(1):20-32. [ Google Scholar]
- Muture BN, Keraka MN, Kimuu PK, Kabiru EW, Ombeka VO, Oguya F. Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: a case control study. BMC Public Health 2011; 11:696. doi: 10.1186/1471-2458-11-696 [Crossref] [ Google Scholar]
- Nugrahaeni DK, Rosmalaningrum L. Risk factors in pulmonary tuberculosis treatment failure. The Indonesian Journal of Public Health 2021; 16(1):12-22. doi: 10.20473/ijph.v16i1.2021.12-22 [Crossref] [ Google Scholar]
- Asres A, Jerene D, Deressa W. Delays to anti-tuberculosis treatment intiation among cases on directly observed treatment short course in districts of southwestern Ethiopia: a cross sectional study. BMC Infect Dis 2019; 19(1):481. doi: 10.1186/s12879-019-4089-x [Crossref] [ Google Scholar]
- Teferi MY, El-Khatib Z, Boltena MT, Andualem AT, Asamoah BO, Biru M. Tuberculosis treatment outcome and predictors in Africa: a systematic review and meta-analysis. Int J Environ Res Public Health 2021; 18(20):10678. doi: 10.3390/ijerph182010678 [Crossref] [ Google Scholar]
- Chen X, Du L, Wu R, Xu J, Ji H, Zhang Y. The effects of family, society and national policy support on treatment adherence among newly diagnosed tuberculosis patients: a cross-sectional study. BMC Infect Dis 2020; 20(1):623. doi: 10.1186/s12879-020-05354-3 [Crossref] [ Google Scholar]
- Mariani H, Afriandi I, Setiawati EP, Gondodiputro S, Wiwaha G, Nataprawira HM. Tuberculosis family support training’s (TB FaST) influence on encouraging TB treatment compliance. Open Public Health J 2022; 15:1-9. doi: 10.2174/18749445-v15-e2208041 [Crossref] [ Google Scholar]
- Izudi J, Tamwesigire IK, Bajunirwe F. Treatment supporters and level of health facility influence completion of sputum smear monitoring among tuberculosis patients in rural Uganda: a mixed-methods study. Int J Infect Dis 2020; 91:149-55. doi: 10.1016/j.ijid.2019.12.003 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Guideline: Nutritional Care and Support for Patients with Tuberculosis. Geneva, Switzerland: WHO; 2013.
- Bhargava A, Benedetti A, Oxlade O, Pai M, Menzies D. Undernutrition and the incidence of tuberculosis in India: national and subnational estimates of the population-attributable fraction related to undernutrition. Natl Med J India 2014; 27(3):128-33. [ Google Scholar]
- Getie A, Alemnew B. Tuberculosis treatment outcomes and associated factors among patients treated at Woldia General Hospital in Northeast Ethiopia: an institution-based cross-sectional study. Infect Drug Resist 2020; 13:3423-9. doi: 10.2147/idr.S275568 [Crossref] [ Google Scholar]
- Pakasi TA, Karyadi E, Wibowo Y, Simanjuntak Y, Suratih NM, Salean M. Vitamin A deficiency and other factors associated with severe tuberculosis in Timor and Rote Islands, East Nusa Tenggara Province, Indonesia. Eur J Clin Nutr 2009; 63(9):1130-5. doi: 10.1038/ejcn.2009.25 [Crossref] [ Google Scholar]
- Kassa GM, Merid MW, Muluneh AG, Fentie DT. Sputum smear grading and associated factors among bacteriologically confirmed pulmonary drug-resistant tuberculosis patients in Ethiopia. BMC Infect Dis 2021; 21(1):238. doi: 10.1186/s12879-021-05933-y [Crossref] [ Google Scholar]