J Educ Community Health. 12(1):11-19.
doi: 10.34172/jech.3369
Original Article
Health Literacy of Hypertensive Patients in a Burkinabe Cardiology Outpatient Clinic
Ahmed Kabore Methodology, Writing – original draft, Writing – review & editing, 1, * 
Laurence Eudoxie Benon Data curation, Investigation, Writing – original draft, Writing – review & editing, 1
Aristide Relwende Yameogo Conceptualization, Methodology, Writing – review & editing, 1, 2
Rayendé Juste Romaric Soubyabiga Formal analysis, Writing – review & editing, 1
Grâce – Alice Enam Bladavi Gumedzoe – Hoseto Data curation, 1
Fasnéwendé Aristide Kabore Supervision, Writing – original draft, Writing – review & editing, 2
Nicolas Meda Conceptualization, Supervision, Writing – original draft, Writing – review & editing, 1, 2
Nobila Valentin Yameogo Conceptualization, Supervision, Writing – original draft, Writing – review & editing, 2
Author information:
1Health Sciences Training and Research Unit (UFR - SDS), Department of Public Health, University Joseph KI ZERBO of Ouagadougou, Burkina Faso
2Health Sciences Training and Research Unit (UFR - SDS), Medicine Section, University of Ouagadougou, Burkina Faso
Abstract
Background: Health literacy (HL) is a multidimensional concept that has become essential for the effective management of chronic diseases. This study aimed to assess the HL of hypertensive patients attending the cardiology outpatient clinic at Yalgado Ouedraogo Teaching Hospital (CHU-YO), Burkina Faso, to propose relevant health promotion interventions.
Methods: This descriptive cross-sectional study was conducted from January to September 2024 on 359 hypertensive outpatients in the cardiology department of CHU-YO. HL levels were measured using the Health Literacy Questionnaire (HLQ).
Results: A total of 359 hypertensive patients with a mean age of 58.12±12.61 years were included. The nine HLQ dimensions were used to assess levels of HL. The lowest scores were found in the dimensions related to the ability to find and evaluate health information, while the highest scores were recorded for social support for health and active engagement with health professionals. A multivariate exploratory cluster analysis method identified LS profiles labeled A to H. Clusters B and G had the lowest HL levels and the greatest health-related challenges, while clusters A, C, F, and H exhibited the highest HL levels.
Conclusion: The ability to find and evaluate health information depends primarily on education level and sources of information. Interventions targeting these two areas are crucial to improve the HL of hypertensive patients. In addition, to reduce inequalities in the care of chronically ill individuals and to inform effective health promotion interventions, cluster analysis is needed to select vulnerable groups.
Keywords: Health education, Cardiovascular diseases, Health literacy questionnaire
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Kabore A, Benon LE, Yameogo AR, Soubyabiga RJR, Gumedzoe – Hoseto GAEB, Kabore FA, et al. Health literacy of hypertensive patients in a burkinabe cardiology outpatient clinic. J Educ Community Health. 2025; 12(1):11-19. doi:10.34172/jech.3369
Introduction
The concept of “health literacy” (hereinafter HL, from the French littératie en santé) is a multidimensional construct. The World Health Organization (WHO) defines HL as a set of cognitive and social skills (e.g., emotional, social, and personal attributes) to help people exercise self-determination in health care, health promotion, and disease prevention (1). It is the generic term for literacy, promoted by the Organization for Cooperation and Development (OECD) in 1995 through a series of publications on adult literacy, including reading and writing skills (2–4). As a result, HL has become the subject of several studies in OECD countries and has attracted increasing interest in low- and middle-income countries. According to Sorensen (5), HL is now recognized as a key determinant of the social, cultural, and environmental factors that shape health outcomes. It has both direct and indirect effects on the health status of individuals and populations. Low levels of HL create many challenges in the management of chronic diseases. These include increased rates of hospitalization, readmission, and mortality, poor understanding of medical prescriptions, lower participation in prevention activities, higher prevalence of health risk factors, limited patient autonomy in managing chronic diseases, less effective communication with health professionals, and increased health care costs (1).
Given these findings, the question arises: how can we best assess the HL levels of individuals or populations? Various tools have been developed to measure aspects of HL, including the European Health Literacy Survey (HLS), which allows for international comparisons. A more recent instrument, the Health Literacy Questionnaire (HLQ), recognizes the multidimensional nature of HL by incorporating scales that measure social dimensions and individuals’ experiences with health professionals (6).
Much of the existing research on HL focuses on measuring average levels and the analysis of factors associated with that level. However, the average scores for the population as a whole do not adequately reflect the diversity of individuals and different groups within the population (7). This interpretation of the data, based on population average scores, leads to fairly comprehensive generalized public health approaches that may exacerbate health inequities. In addition to general population-level measures, analyses should also focus on the needs of specific groups, particularly those who are marginalized and disadvantaged. One method used for this purpose is hierarchical cluster analysis. The HLQ is well-suited to this kind of analysis and has been widely used in various countries with health disparities, particularly within the African region. In some of these countries, a local adaptation of the tool has been developed or is currently underway. This approach to HL is widely used in the Optimization Health Literacy and Access (OPHELIA) process, which advocates a three-phase framework for implementing coherent universal and specific interventions (8).
High blood pressure (HTN) is currently the most prevalent chronic disease globally (9). According to the WHO, it affects approximately one in three adults or about 1.3 billion people aged 30 to 79 years worldwide. It is one of the major risk factors for cardiovascular diseases and causes approximately 18 million deaths annually worldwide. It remains the leading cause of death worldwide (10).
Burkina Faso, like many other low- and lower-middle-income countries, is marked by the burden of non-communicable diseases (NCDs), particularly HTN. The WHO Global Report on Hypertension (2023) revealed a prevalence rate of 31% in 2019 for HTN among adults aged 30-79, affecting approximately 1.5 million individuals (11). Additionally, the 2021 STEPS Country Survey reported an 18.2% prevalence of HTN among people aged 18-69 years (12).
To address this, the Ministry of Health of Burkina Faso created a dedicated directorate for the prevention and control of NCDs (13). Regarding HTN, the national strategy aligns with the WHO’s HEARTS and PEN programs in the African regions which promote the decentralization of primary healthcare services.
This study is the first to investigate HL in patients with HTN in Burkina Faso. Its findings can help design targeted interventions to improve disease management.
Materials and Methods
Type of Study
A cross-sectional descriptive study was conducted from January to September 2024.
Study Site
The study was conducted in the cardiology outpatient clinic of the University Hospital Yalgado Ouedraogo (CHU-YO) in Ouagadougou, Burkina Faso.
Data Collection Technique and Tools
Data were collected by trained interviewers through structured face-to-face individual interviews using a collection sheet with two main components:
-
A general survey, designed to collect socio-demographic and clinical characteristics of patients.
-
The HLQ is a validated instrument consisting of 44 items. It is subdivided into two parts: the first part measures dimensions 1 to 5, and the part covers dimensions 6 through 9. These dimensions are evaluated using Likert-scale items.
The HLQ includes the following nine areas:
-
Feeling understood and supported by healthcare providers
-
Having enough information to manage health
-
Actively managing one’s health
-
Social support for health
-
Assessment of health information
-
Ability to actively collaborate with healthcare providers
-
Navigating the healthcare system
-
Ability to find good health information
-
Understand health information well enough to know what to do.
The nine domains comprise a total of 44 elements, with each domain comprising four or five elements.
Domains 1 to 5 are scored on a 4-point Likert scale, with response options ranging from “not at all” (1) to “Totally agree” (4). These dimensions reflect participants’ beliefs about the availability of resources for managing their health. Domains 6 to 9 are scored on a 5-point Likert scale from ‘impossible or always difficult” (1) to “always easy” (5). These dimensions assess participants’ beliefs about the ease or difficulty of tasks described in the specific domains. Each item is presented as a statement and the participants are asked to choose the response that best reflects their current situation.
After applying for a license agreement to use the HLQ questionnaire from Professor Osborne, we obtained an already-translated version from the original English to French. Before collecting data in real situations, we conducted a pre-test to assess patients’ understanding of the questionnaire items and to evaluate the performance of the data collection tools and techniques.
Reproducibility and Quality of Study
After obtaining a license to use the HLQ questionnaire from Professor Osborne, a translated version from English to French was made available. To improve the data collection process, a pre-test was administered to both non-schooled patients (using a local language translation) to detect possible complexities in understanding and some schooled patients in French. This pre-test allowed us to adapt the questionnaire according to the patient’s educational status and level of understanding.
Data Sources
Hypertensive patients seen in the CHU-YO cardiology outpatient clinic constituted the source population. Patient records and medical files were also used to collect data.
Criteria for Inclusion
Patients need to be hypertensive, be at least 30 years old, have been followed in the CHU-YO cardiology department for at least six months, and agree to participate in the study.
Sampling Methods and Techniques
Sampling
A comprehensive sampling approach was used.
Sample Size
According to the WHO Global Report on HTN in 2023, the prevalence of this disease in Burkina Faso among adults aged 30-79 years was 31% in 2019 (11). Using the OPEN EPI application version 3 and Schwartz’s formula, the sample size was calculated as follows:
Where,
z = 1.96 for a 95% confidence interval
p = 0.31 proportion of HTNs in the population
q = 1-p = 0.69
i = 0.05 (margin of error)
Data Analysis and Processing
Data were analyzed using IBM SPSS Statistics version 25. An epidemiological description was followed by a multivariate or hierarchical cluster analysis to identify clusters within the sample.
Formation of Clusters
Cluster analysis is a statistical technique used to group individuals with similar characteristics. It is used to identify homogeneous profiles within a population. In our study, Euclidean distance was used as the measure of similarity. This distance calculates the difference between individuals’ scores to evaluate their proximity. The smaller the Euclidean distance between two individuals, the more similar the level of HL.
To group individuals, we applied hierarchical classification, which organizes individuals into groups in a stepwise manner. Initially, each individual is treated as a single group, and then the most similar individuals are merged successively until several distinct clusters are formed.
Hierarchical Classification
Hierarchical classification is a grouping technique that organizes individuals based on their statistical proximity. It relies on a distance matrix, which compares each individual with others to identify similarities between them.
To form clusters, we used an aggregation method to determine how individuals are merged at each step. Among the various available methods exist, we selected the Ward method, which minimizes the variance within each group. This method is widely preferred because it produces well-balanced and coherent clusters, thus facilitating their interpretation.
Using this approach, we were able to group students according to their HL level, enabling a better analysis of disparities and the factors influencing these levels.
Definition of Indicators
The indicators used in this study were:
-
Average scores were obtained on the nine scales of the HLQ to assess the overall level of HL in the sample.
-
Six levels of HL were found, including very high (dark green), High (light green), Good (light yellow), Fairly good (mustard), Low (pink), and very low (red).
-
Eight identified clusters, labeled A, B, C, D, E, F, G, and H were found.
Ethical and Deontological Aspects
To conduct the study, ethical approval was obtained from the Ethics Committee under reference number 2024-04-112. The research protocol was submitted to the CHU-YO management for authorization. Each participant received an explanation of the study’s objectives to ensure a sufficient understanding of our study topic. A consent form was provided to participants. Authorization from participants was obtained prior to the interview. Participation was voluntary and documented by signing a free, informed, and individual consent form. The anonymity of participants was guaranteed, as no confidential information that can identify patients was collected or stored.
Results
Sociodemographic and Clinical Characteristics of the Sample
A total of 359 hypertensive patients attending the CHU-YO cardiology outpatient clinic were included in the study. Table 1 presents the frequency of participants categorized by sociodemographic and clinical characteristics.
Table 1.
Sociodemographic and Clinical Characteristics of Hypertensive Patients
|
Features
|
Size
|
Percent
|
| Sex |
|
|
| Male |
108 |
30.08 |
| Female |
251 |
69.92 |
| Age group (y) |
|
|
| 30-45 |
60 |
16.71 |
| 46-60 |
143 |
39.83 |
| ≥ 61 |
156 |
43.46 |
| Socio-occupational categories |
|
|
| Informal sector |
28 |
7.80 |
| Merchant |
35 |
9.75 |
| Employee |
68 |
18.94 |
| Housewife |
124 |
34.54 |
| Unemployed |
8 |
2.23 |
| Retired |
82 |
22.84 |
| Farmer/Grower |
14 |
3.9 |
| Marital status |
|
|
| Single |
93 |
25.91 |
| In a relationship |
266 |
74.09 |
| Features |
Size |
|
| Residential environment |
|
|
| Urban |
323 |
89.94 |
| Rural |
36 |
10.06 |
| Level of education |
|
|
| Literate |
17 |
4.74 |
| Primary |
73 |
20.61 |
| Secondary |
96 |
26.74 |
| Higher education |
53 |
14.76 |
| No formal education |
120 |
33.43 |
| Perception of socio-economic status |
| High |
7 |
1.90 |
| Average |
197 |
54.9 |
| Low |
155 |
43.2 |
| Body mass index |
|
|
| Underweight |
5 |
1.39 |
| Normal |
116 |
32.31 |
| Overweight/Obese |
238 |
66.29 |
| HTN duration (months) |
|
|
| 6-12 |
49 |
13.65 |
| 12-60 |
89 |
24.79 |
| 60-120 |
82 |
22.84 |
| ≥ 120 |
139 |
38.72 |
| Tobacco use |
|
|
| Yes |
8 |
2.23 |
| No |
351 |
97.77 |
| Diabetes |
|
|
| Yes |
70 |
19.5 |
| No |
289 |
80.5 |
| Obesity |
|
|
| Yes |
238 |
66.3 |
| No |
121 |
33.7 |
| Age FRCV |
|
|
| Yes |
229 |
63.79 |
| No |
130 |
36.21 |
| Menopause |
|
|
| Yes |
13 |
3.62 |
| No |
346 |
96.38 |
| Target voltage achieved |
|
|
| Yes |
209 |
58.06 |
| No |
151 |
41.94 |
| Sedentary lifestyle |
|
|
| Yes |
176 |
49.03 |
| No |
183 |
50.97 |
| Family TCCA |
|
|
| Yes |
61 |
16.99 |
| No |
298 |
83.01 |
| Psychosocial rist factors |
|
|
| Yes |
60 |
16.71 |
| No |
299 |
83.29 |
Note. HTN: Hypertension; FRCV: Cardiovascular risk factors, TCCA: Associated cardiac and cerebral conditions.
Health Literacy Levels Among Hypertensive Patients
In the first part of the HLQ, the highest average score was observed in Dimension 4: Social Support for Health (mean = 3.11), while the lowest was in Dimension 5: Evaluation of Health Information (mean = 2.25). In the second part, the highest average score was found in Dimension 6: Ability to actively engage with health professionals (mean = 3.68). Conversely, the lowest score was recorded in Dimension 8: Ability to find good health information (mean = 3.02), highlighting a key area of difficulty (Table 2). Figure 1 shows the distribution of hypertensive patients according to scores obtained across the nine dimensions of the HLQ.
Table 2.
Average Scores for the Nine Dimensions of the Health Literacy Questionnaire
|
HLQ Scale
|
Average (SD) (95% CI)
|
|
Range 1 (lowest) -4 (highest)
|
| 1. Feel understood and supported by health professionals |
2.80 (0.63) [2.73 - 2.86] |
| 2. Have sufficient information to manage my health |
2.33 (0.55) [2.27 – 2.38] |
| 3. Actively manage my health |
2.88 (0.41) [2. 83 – 2.92] |
| 4. Social support for health |
3.11 (0.50) [3.05 – 3.16] |
| 5. Evaluation of health information |
2.25 (0.64) [2.18 – 2.32] |
|
|
Range 1 (lowest) -5 (highest)
|
| 6. Ability to actively engage with health professionals |
3.68 (0.60) [3.62 – 3.74] |
| 7. Navigating the healthcare system |
3.10 (0.55) [3.04 – 3.15] |
| 8. Ability to find good health information |
3.02 (0.80) [2.93 – 3.10] |
| 9. Understand health information well enough to know what to do |
3.20 (0.96) [3.10 - 3.30] |
Note. SD: Standard deviation; CI: Confidence interval.
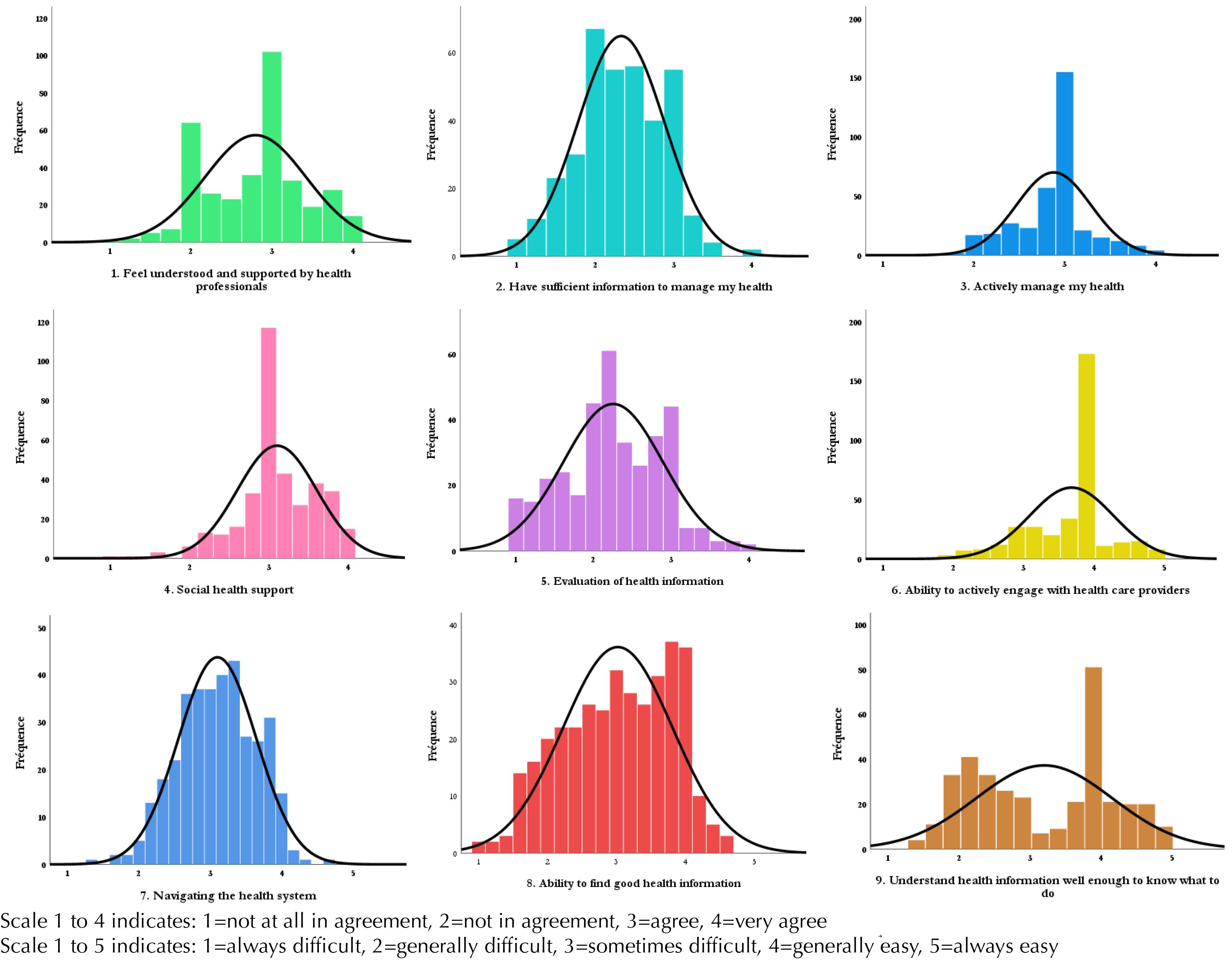
Figure 1.
Distribution of Hypertensive Patients Across the Nine Dimensions of Health Literacy
.
Distribution of Hypertensive Patients Across the Nine Dimensions of Health Literacy
Different Profiles or Specific Groups of Health Literacy Characteristics Within the Sample
The exploratory multivariate cluster analysis identified eight distinct HL profiles within the study sample, each characterized by specific sociodemographic and clinical attributes. Table 3 describes the sociodemographic and clinical characteristics specific to each cluster.
Table 3.
Sociodemographic and Medical Characteristics Associated With Clusters
|
|
Clusters
|
|
A
|
B
|
C
|
D
|
E
|
F
|
G
|
H
|
| Number of participants (%) |
9.40 |
12.20 |
20.30 |
18.60 |
10.30 |
10.30 |
12.50 |
6.40 |
| Socio-demographic characteristics |
|
|
|
|
|
|
|
|
| Average age (years) |
59.41 |
60.36 |
55.059 |
57.4 |
59.73 |
59.19 |
60.84 |
52.39 |
| Male (%) |
23.5 |
29.5 |
30.1 |
23.9 |
35.1 |
43.2 |
28.9 |
30.4 |
| Occupation: Informal sector (%) |
5.9 |
29.5 |
8.2 |
34.3 |
32.4 |
5.4 |
31.1 |
21.7 |
| Occupation: Employee (%) |
20.6 |
0 |
41.1 |
6 |
5.4 |
43.2 |
2.2 |
34.8 |
| Occupation: Housewife (%) |
35.3 |
54.5 |
17.8 |
41.8 |
43.2 |
8.1 |
53.3 |
17.4 |
| Occupation: Unemployed/ Retired (%) |
38.2 |
15.9 |
32.9 |
17.9 |
18.9 |
43.2 |
13.3 |
26.1 |
| Marital Status: In a relationship (%) |
29.4 |
27.3 |
28.8 |
25.4 |
29.7 |
13.5 |
33.3 |
8.7 |
| Urban Residence (%) |
97.1 |
86.4 |
94.5 |
92.5 |
83.8 |
89.2 |
75.6 |
100 |
| Secondary education level or above (%) |
58.8 |
0 |
79.5 |
25.4 |
10.8 |
94.6 |
4.4 |
60.9 |
| Perceived average or high socioeconomic level (%) |
73.5 |
27.3 |
84.9 |
59.7 |
24.3 |
78.4 |
26.7 |
73.9 |
| Medical conditions |
|
|
|
|
|
|
|
|
| Age of HTN between 6 and 12 months (%) |
8.8 |
31.8 |
9.6 |
7.5 |
21.6 |
5.4 |
8.9 |
30.4 |
| Age of HTN between 12 and 60 months (%) |
26.5 |
18.2 |
21.9 |
25.4 |
29.7 |
24.3 |
31.1 |
21.7 |
| Age of HTN between 60 and 120 months (%) |
147 |
20.5 |
31.5 |
23.9 |
13.5 |
24.3 |
26.7 |
13 |
| The seniority of HTN over 120 months (%) |
50 |
29.5 |
37 |
43.3 |
35.1 |
45.9 |
33.3 |
34.8 |
| Body mass index: Overweight (%) |
64.7 |
61.4 |
69.9 |
68.7 |
48.6 |
83.8 |
55.6 |
78.3 |
| Consumption of tobacco (%) |
0 |
2.3 |
5.5 |
3 |
0 |
2.7 |
0 |
0 |
| Diabetes (%) |
14.7 |
13.6 |
21.9 |
16.4 |
21.6 |
32.4 |
15.6 |
21.7 |
| Age cardiovascular risk factor (%) |
26.5 |
34.1 |
32.9 |
26.9 |
35.1 |
43.2 |
31.1 |
34.8 |
| Sedentary (%) |
47.1 |
45.5 |
54.8 |
58.2 |
37.8 |
54.1 |
55.6 |
8.7 |
| Family history of cardiovascular disease (%) |
23.5 |
13.6 |
20.5 |
13.4 |
18.9 |
16.2 |
17.8 |
13 |
| Psychosocial and socio-economic factors (%) |
11.8 |
18.2 |
13.7 |
10.4 |
32.4 |
13.5 |
22.2 |
17.4 |
| Achievement of target tensile strength (%) |
61.8 |
45.5 |
65.8 |
56.7 |
54.1 |
62.2 |
48.9 |
73.9 |
Specific Cluster Health Literacy Strengths and Weaknesses
Clusters A, C, F, and H exhibit the highest levels of HL across most dimensions, while clusters B and G indicate the lowest levels. Table 4 presents the specific groups categorized by their HL scores across the nine dimensions.
Table 4.
Cluster Analysis of Eight Health Competency Clusters
|
|
Clusters
|
|
A
|
B
|
C
|
D
|
E
|
F
|
G
|
H
|
| Number of participants |
9.40 |
12.20 |
20.30 |
18.60 |
10.30 |
10.30 |
12.50 |
6.40 |
| Within the cluster HLQ (SD) average score |
|
|
|
|
|
|
|
|
| 1. Feel understood and supported by health care providers |
3.23 |
2.34 |
3.07 |
2.34 |
3.17 |
3.28 |
2.26 |
3.17 |
| 0.70 |
0.64 |
0.32 |
0.41 |
0.40 |
0.42 |
0.42 |
0.39 |
| 2. Have sufficient information to manage my health |
2.94 |
1.85 |
2.53 |
2.22 |
1.74 |
3.02 |
1.89 |
2.74 |
| 0.25 |
0.44 |
0.34 |
0.33 |
0.34 |
0.32 |
0.38 |
0.21 |
| 3. Actively manage my health |
3.50 |
2.28 |
2.90 |
2.94 |
2.89 |
2.96 |
2.94 |
2.58 |
| 0.32 |
0.31 |
0.35 |
0.21 |
0.40 |
0.26 |
0.12 |
0.22 |
| 4. Social health support |
3,44 |
3.18 |
3.04 |
2.69 |
3.45 |
3.12 |
2.85 |
3.81 |
| 0.42 |
0.56 |
0.23 |
0.54 |
0.26 |
0.38 |
0.37 |
0.16 |
| 5. Evaluation of health information |
2.55 |
1.71 |
2.55 |
2.22 |
1.48 |
3.10 |
1.82 |
2.74 |
| 0.63 |
0.43 |
0.39 |
0.36 |
0.35 |
0.37 |
0.49 |
0.32 |
| 6. Ability to actively engage with health care providers |
4.36 |
2.63 |
3.81 |
3.82 |
3.74 |
4.15 |
3.32 |
3.80 |
| 0.35 |
0.45 |
0.38 |
0,.24 |
0.37 |
0.33 |
0.45 |
0.31 |
| 7. Navigating the health system |
3.54 |
2.33 |
3.37 |
3.06 |
2.77 |
3.87 |
2.73 |
3.17 |
| 0.34 |
0.37 |
0.33 |
0.37 |
0.33 |
0.26 |
0.27 |
0.25 |
| 8. Ability to find good health information |
3.64 |
2.02 |
3.66 |
3.08 |
2.20 |
3.96 |
2.30 |
3.00 |
| 0.47 |
0.48 |
0.33 |
0.36 |
0.48 |
0.32 |
0.47 |
0.46 |
| 9. Understand health information well enough to know what to do |
3.74 |
2.00 |
3.83 |
2.97 |
2.86 |
4.17 |
2.24 |
4.31 |
| 0.77 |
0.38 |
0.57 |
0.73 |
0.79 |
0.38 |
0.30 |
0.28 |
Note. HLQ: Health literacy questionnaire; SD: Standard deviation.
Discussion
Recalls of Key Results
A total of 359 hypertensives patients were included in our study, with a mean age of 58.12 + /- 12.61 years. The nine dimensions of the HLQ provided valuable insights into the HL strengths and needs of the study population. The overall level of HL in the sample was adequate, as all average scores across the nine dimensions were above average. The lowest scores were observed in the ability to find good health information and evaluate it, and the highest scores were in social support for health and the ability to actively engage with healthcare professionals. The multivariate exploratory cluster analysis identified distinct HL profiles, labeled from A to H. Clusters B and G had the lowest levels of HL and faced the greatest challenges, whereas clusters C, F, and H exhibited the highest HL levels across the most dimensions.
Limits
Several limitations and biases affected the implementation of our study. We used a convenience sampling method, which limits the generalizability of our results to the broader HTN population. The cross-sectional nature of this study inevitably introduced memory recall and social desirability biases. Despite these limitations, we have achieved actionable results that have been critically interpreted.
The HLQ is a tool for assessing HL, but it does not provide a single overall score due to the multidimensional nature of the concept.
Gaps and Challenges in the Ability to Find and Evaluate Good Health Information
In our study, the overall population demonstrated an adequate HL level because all average scores across the nine HLQ dimensions were above average. However, a more detailed analysis revealed significant weaknesses in the domains related to the ability to find and evaluate good health information.
An individual’s capacity to locate and assess health information depends on several personal, socio-economic, and environmental factors, especially on their sources of information (14,15). In our context, this limited ability is largely linked to low levels of education among participants (16). Specifically, 38.16% of the hypertensive patients surveyed had an education level below primary school. In addition, the low socio-economic status of the sample, comprising mostly retired, elderly individuals and housewives, contributed to this weakness (16).
The relatively advanced age of participants may also help explain these difficulties. About 43% of the study population was over 60 years old. In our context, most older individuals rely primarily on family members, complementary or alternative medicine practitioners, and health workers as their main sources of information to manage their health (17). A study conducted of hypertensive patients in Ghana reported that 70% of alternative medicine users did not inform their health professionals of their use, citing fear and a lack of information or guidance from healthcare providers as the main reasons for nondisclosure (18).
Today, the internet has become the world’s leading source of health information, but it is not always affordable for our people (19). More than two-thirds of people in developed countries search for health information online (20). Although online health information-seeking behavior has increased in low- and middle-income countries (FPR-I) due to increased smartphone use and the development of information technologies and social media, access remains limited (14). In summary, this limited access to health information and challenges in evaluating it represent a major obstacle to the empowerment of hypertensive patients in managing their own disease. The improvement and development of sources of information from associations and non-profit organizations for HTN people, perhaps via radio and television, are thus necessary.
This finding is comparable with that of Passi et al, who in their work on a rural population in India in 2023 (14) found that individuals with lower secondary education had difficulties accessing, understanding, and evaluating health information. Similarly, Anwar et al in Egypt in 2020 (21), in a study of underserved populations, showed that people without access to the Internet were at a significant disadvantage in accessing health services and using them effectively. The links among internet access, higher education, and literacy reflect the strong associations among almost all HLQ dimensions and education levels. Moreover, numerous studies on the level of HL among populations with chronic disease conditions have also noted weaknesses in the dimension of access to health information.
Given this fact, we recommend that governments and policymakers in low-resource countries prioritize the improvement of health information sources to raise the HL level of HT patients (1).
The Strength of Social Capital and Engagement With Health Professionals
Detailed analysis of the average scores across the nine HLQ scales also found that the highest HL levels were related to social support for health and the ability to actively engage with health professionals.
According to the literature, membership in a social organization is associated with a higher probability of HTN detection and control (22). Social capital, community safety, and interpersonal relationships are important factors in protecting the health status of patients with chronic diseases. Establishing a safe community environment and fostering interpersonal networks contribute to better patient outcomes (23). Despite the deterioration of social and family structures in many areas, patients with chronic conditions in Africa benefit from social capital to help manage their disease. This likely explains why our study population reported receiving social support. The chronic conditions in our study population may also motivate patients to engage actively with healthcare providers.
This social contribution is of great importance in health promotion, as it can serve as a foundation for community health interventions. Several studies measuring HL among patients with chronic diseases the HLQ demonstrated the significant impact of social capital (14). However, in their 2019 study in Australia, Rheault et al were surprised to observe low levels of perceived social health support (24).
Social capital remains a cornerstone in the management of chronic diseases. We recommend that families and societies in poor countries work to strengthen the capital to improve the management of chronic diseases, especially HTN.
Clusters in Health Literacy and Health Inequity
The exploratory multivariate cluster analysis identifies HL profiles labeled A, B, C, D, E, F, G, and H. Clusters B and G exhibited the greatest challenges in terms of HL, as reflected by their very low average scores in several HLQ dimensions: the provision of sufficient information for health, the ability to find good health information, understanding what health information is needed and how it should be used, assessing health information, and guiding the healthcare system. The low HL observed in clusters B and G appears to be multifactorial and probably related to their sociodemographic and clinical characteristics. These groups were predominantly made up of elderly patients (over 60 years old), mostly unemployed housewives, with low levels of education and socioeconomic status. In addition, these clusters had the lowest levels of HTN control. Evidence indicates that women from FPR-I often have limited autonomy and control over their health-related decisions (25). This situation is marked in our study regarding the above-mentioned precarious conditions.
Low levels of HL affect people’s health not only because they lack the means to understand health messages, but also because they have reduced opportunities for social and cultural participation (1). In public health, this group is characterized by significant challenges arising from inequalities and disparities in health, which hinder the effective use of health services, specifically in terms of cost, participation, empowerment, and sustainability. The OPHELIA process was initiated to identify such vulnerable populations (phase 1) and to design health promotion interventions at various levels based on their active participation (13). These interventions may include awareness and information sessions aimed at behavior change, therapeutic education, and the creation of associations or clubs for hypertensive patients to provide frameworks for exchange and support (15). At the policy and decision-making levels, interventions can include large-scale implementation of the WHO’s decentralization programs at the basic levels through PEN and HEARTS, as well as ensuring access to affordable generic drugs for all. Additionally, measures are needed to improve the accessibility of health information and services, along with training programs for professionals adapted to address issues related to HL. In summary, according to Ferron’s analysis (1), two types of recommendations are appropriate:
-
Implementation of health promotion interventions that reach the entire population and are based on universalism.
-
Implementation of targeted measures tailored to the specific needs of certain population groups.
Our results are similar to those of Passi et al, who found that patients with the lowest socioeconomic status had the lowest health culture scores (14).
Conclusion
Our study revealed weaknesses in HL among the hypertensive population attending the cardiology outpatient clinic at CHU-YO. Examining participant characteristics enables us to categorize the population in order to target the most vulnerable individuals experiencing serious health disparities and inequalities for urgent health promotion interventions. Improving the HL of hypertensive patients is therefore an essential strategy to fight this disease. Indeed, HL has become a major determinant of health and must be integrated into public health policies.
As perspectives for this study, we intend to evaluate the information sources utilized by hypertensive patients and propose concrete health promotion interventions such as therapeutic education for HTN. Furthermore, discussions will explore the establishment of communication frameworks for hypertensive patients using advanced communication technologies. Extending this research to rural areas would be highly valuable, especially in supporting the decentralization of HTN management within primary healthcare frameworks (e.g., HEARTS and PEN programs).
Competing Interests
The authors have no competing interests associated with the material presented in this article.
Funding
None.
References
- Ferron C. La Littératie en Santé: Synthèse Bibliographique. Aubervilliers, FR: Fnes; 2017.
- Organisation for Economic Co-operation and Development (OECD), Statistics Canada. Literacy, Economy and Society: Results of the First International Adult Literacy Survey. Ottawa, Ontario: Statistics Canada; 1995. p. 72.
- Organisation for Economic Co-operation and Development (OECD), Statistics Canada. Literacy and the Knowledge Society: New Results from the International Adult Literacy Survey. Paris: OECD; 1997. p. 212.
- Organisation for Economic Co-operation and Development (OECD), Statistics Canada. Literacy in the Information Age: Final Report of the International Adult Literacy Survey. Paris: OECD; 2000. p. 211.
- Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health 2012; 12:80. doi: 10.1186/1471-2458-12-80 [Crossref] [ Google Scholar]
- Osborne RH, Cheng CC, Nolte S, Elmer S, Besancon S, Budhathoki SS. Health literacy measurement: embracing diversity in a strengths-based approach to promote health and equity, and avoid epistemic injustice. BMJ Glob Health 2022; 7(9):e009623. doi: 10.1136/bmjgh-2022-009623 [Crossref] [ Google Scholar]
- Mantwill S, Monestel-Umaña S, Schulz PJ. The relationship between health literacy and health disparities: a systematic review. PLoS One 2015; 10(12):e0145455. doi: 10.1371/journal.pone.0145455 [Crossref] [ Google Scholar]
- Beauchamp A, Batterham RW, Dodson S, Astbury B, Elsworth GR, McPhee C. Systematic development and implementation of interventions to optimise health literacy and access (Ophelia). BMC Public Health 2017; 17(1):230. doi: 10.1186/s12889-017-4147-5 [Crossref] [ Google Scholar]
- World Health Organization (WHO). First WHO Report Details Devastating Impact of Hypertension and Ways to Stop it. WHO; 2023.
- Santé OM de la. Développement de la littératie en santé pour la prévention et le contrôle des maladies non transmissibles: Volume 2. Une perspective pertinente à l’échelle mondiale; 2022. p. 54.
- World Health Organization (WHO). Global Report on Hypertension: The Race Against a Silent Killer. Geneva: WHO; 2023. p. 291.
- Institut National de la Statistique et de la Démographie U The DHS Program ICF Rockville, Maryland. Enquête Démographique et de Santé et indicateurs clés du Burkina Faso 2021. 2022.
- World Health Organization (WHO). Burkina Faso: Créer de Nouveaux Outils Pour Agir Sur L’hypertension. WHO; 2020.
- Passi R, Kaur M, Lakshmi PVM, Cheng C, Hawkins M, Osborne RH. Health literacy strengths and challenges among residents of a resource-poor village in rural India: epidemiological and cluster analyses. PLOS Glob Public Health 2023; 3(2):e0001595. doi: 10.1371/journal.pgph.0001595 [Crossref] [ Google Scholar]
- Joshi H, Kalauni BR, Bhusal K, Bhandari R, Subedi A, Bhandari B. Health literacy among patients with non-communicable diseases at a tertiary level hospital in Nepal-a cross sectional study. PLoS One 2024; 19(6):e0304816. doi: 10.1371/journal.pone.0304816 [Crossref] [ Google Scholar]
- Heijmans M, Waverijn G, Rademakers J, van der Vaart R, Rijken M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ Couns 2015; 98(1):41-8. doi: 10.1016/j.pec.2014.10.006 [Crossref] [ Google Scholar]
- Özkan S, Tüzün H, Dikmen AU, Aksakal NB, Çalışkan D, Taşçı Ö. The relationship between health literacy level and media used as a source of health-related information. Health Lit Res Pract 2021; 5(2):e109-17. doi: 10.3928/24748307-20210330-01 [Crossref] [ Google Scholar]
- Kretchy IA, Owusu-Daaku F, Danquah S. Patterns and determinants of the use of complementary and alternative medicine: a cross-sectional study of hypertensive patients in Ghana. BMC Complement Altern Med 2014; 14:44. doi: 10.1186/1472-6882-14-44 [Crossref] [ Google Scholar]
- Renahy E, Parizot I, Chauvin P. Determinants of the frequency of online health information seeking: results of a web-based survey conducted in France in 2007. Inform Health Soc Care 2010; 35(1):25-39. doi: 10.3109/17538150903358784 [Crossref] [ Google Scholar]
- Jia X, Pang Y, Liu LS. Online health information seeking behavior: a systematic review. Healthcare (Basel) 2021; 9(12):1740. doi: 10.3390/healthcare9121740 [Crossref] [ Google Scholar]
- Anwar WA, Mostafa NS, Hakim SA, Sos DG, Abozaid DA, Osborne RH. Health literacy strengths and limitations among rural fishing communities in Egypt using the Health Literacy Questionnaire (HLQ). PLoS One 2020; 15(7):e0235550. doi: 10.1371/journal.pone.0235550 [Crossref] [ Google Scholar]
- Palafox B, Goryakin Y, Stuckler D, Suhrcke M, Balabanova D, Alhabib KF. Does greater individual social capital improve the management of hypertension? Cross-national analysis of 61 229 individuals in 21 countries. BMJ Glob Health 2017; 2(4):e000443. doi: 10.1136/bmjgh-2017-000443 [Crossref] [ Google Scholar]
- Xia J, Wu NW, Yu C, Li NX. [Influence of social capital on the life quality of patients with chronic diseases-a study based on EQ-5D-5L scale]. Sichuan Da Xue Xue Bao Yi Xue Ban 2021; 52(5):778-82. doi: 10.12182/20210960505 [Crossref] [ Google Scholar]
- Rheault H, Coyer F, Jones L, Bonner A. Health literacy in Indigenous people with chronic disease living in remote Australia. BMC Health Serv Res 2019; 19(1):523. doi: 10.1186/s12913-019-4335-3 [Crossref] [ Google Scholar]
- Sougou NM, Sougou AS, Bassoum O, Lèye MM, Faye A, Seck I. Factors associated with women’s decision-making autonomy for their health in Senegal. Sante Publique 2020; 32(4):381-8. doi: 10.3917/spub.204.0381 [Crossref] [ Google Scholar]