J Educ Community Health. 12(2):100-109.
doi: 10.34172/jech.3436
Original Article
Theoretically Planned Intervention for Head Lice Infestation Prevention Among Students: An Integrated Health Belief Model Approach
Atefeh Koulivand Data curation, Investigation, Resources, Writing – original draft, 1 
Sakineh Rakhshanderou Formal analysis, Software, Validation, Writing – review & editing, 1
Parisa Hosseini Koukamari Methodology, Visualization, Writing – original draft, Writing – review & editing, 2
Mohtasham Ghaffari Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing, 1, *
Author information:
1School of Public Health & Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran
Abstract
Background: This study aimed to evaluate the effectiveness of an educational intervention grounded in the Integrated Health Belief Model (IHBM) in promoting preventive behaviors among female primary school students.
Methods: In the present interventional research, primary school students were randomly assigned to intervention (n=69) and control (n=69) groups. Data collection was carried out using a questionnaire that included demographic information and IHBM constructs. The intervention consisted of six educational sessions conducted for students in the intervention group using lectures, video presentations, group discussions, and role-playing techniques. Both groups were assessed at three stages: pre-test, immediate post-test, and two months after the intervention. The data were analyzed using chi-square, Mann-Whitney, and Wilcoxon tests via SPSS software Version 16.
Results: In both the immediate post-intervention assessment and the two-month follow-up, the intervention group showed a significant increase in mean scores for knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived self-efficacy, preventive behaviors, and social support compared to the control group (P<0.05). However, the mean score for reinforcement did not show a statistically significant change after the intervention (P>0.05).
Conclusion: The results of the present study highlight the effectiveness of educational interventions in enhancing knowledge, perceived susceptibility, severity, benefits, barriers, self-efficacy, social support, and preventive measures against head lice infestations. The findings suggest the need for designing and implementing theory-based programs to prevent and control school pediculosis.
Keywords: Intervention, Head lice infestation, Student, Integrated health belief model
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Koulivand A, Rakhshanderou S, Hosseini Koukamari P, Ghaffari M. Theoretically planned intervention for head lice infestation prevention among students: an integrated health belief model approach. J Educ Community Health. 2025; 12(2):100-109. doi:10.34172/jech.3436
Introduction
Pediculosis, commonly known as head lice infestation, is a significant global public health issue that affects millions of individuals worldwide and represents a common parasitic infestation (1). Managing and treating pediculosis imposes a considerable financial burden on public health resources, particularly in underdeveloped and developing countries where healthcare funding is often limited and constrained (2).
Approximately 19% of school-aged children are affected by pediculosis capitis, with girls being 2.5 times more susceptible than boys (3). Aligns with global patterns; a systematic review in Iran found that the incidence of head lice among girls is 4.5 times greater than in boys (4), with regional prevalence ranging from 2.3% to 17.5% (5-8). Similar findings have been reported in studies conducted in several countries, including Argentina (9), Syria (10), Thailand (11), and Turkey (12).
Gender-related behavioral differences, such as maintaining closer contact in small gatherings (3), longer hair length, and direct contact with an infected person, contribute to the increased prevalence of pediculosis among girls. However, lice can also spread through contaminated personal objects such as bedding, pillows, and hair accessories (13). Additional factors, including the frequency of hair washing, awareness of lice, and high environmental density, can further facilitate the transmission of head lice (14). Therefore, disrupting the transmission cycle is essential to effectively prevent and control school-based pediculosis.
Head lice prevention can be achieved through well-structured health education programs, in which the selection of a suitable theoretical framework plays a critical role. The Health Belief Model (HBM) is a widely recognized psychosocial approach that effectively predicts an individual’s likelihood of adopting preventive measures (15). According to the HBM, the adoption of pediculosis-preventive behaviors among students depends on perceived susceptibility (students perceive themselves to be infested), perceive severity (understanding the seriousness of the condition), perceived benefits (belief in the efficacy of preventive behaviors), perceived barriers (believing that preventive behaviors are manageable), and perceived self-efficacy (belief in one’s ability to perform the preventive actions) (16).
This study employs the HBM to address pediculosis prevention, focusing on key determinants such as awareness, family support, and encouragement (17). Previous research has shown that this model effectively promotes preventive behaviors, with social support playing a vital role in shaping health-related outcomes (18,19). Moreover, reinforcement mechanisms can increase the likelihood of repeating positive health behaviors (20). Given the greater vulnerability of young girls to pediculosis and the urgent need to design, implement, and evaluate effective preventive educational programs in school-aged populations, this study was carried out to examine the influence of health education intervention on head lice-related preventive behaviors among primary school students. Accordingly, an intervention grounded in the Integrated Health Belief Model (IHBM) was designed (See Figure 1) to evaluate its efficacy in promoting preventive behaviors against pediculosis in this population.
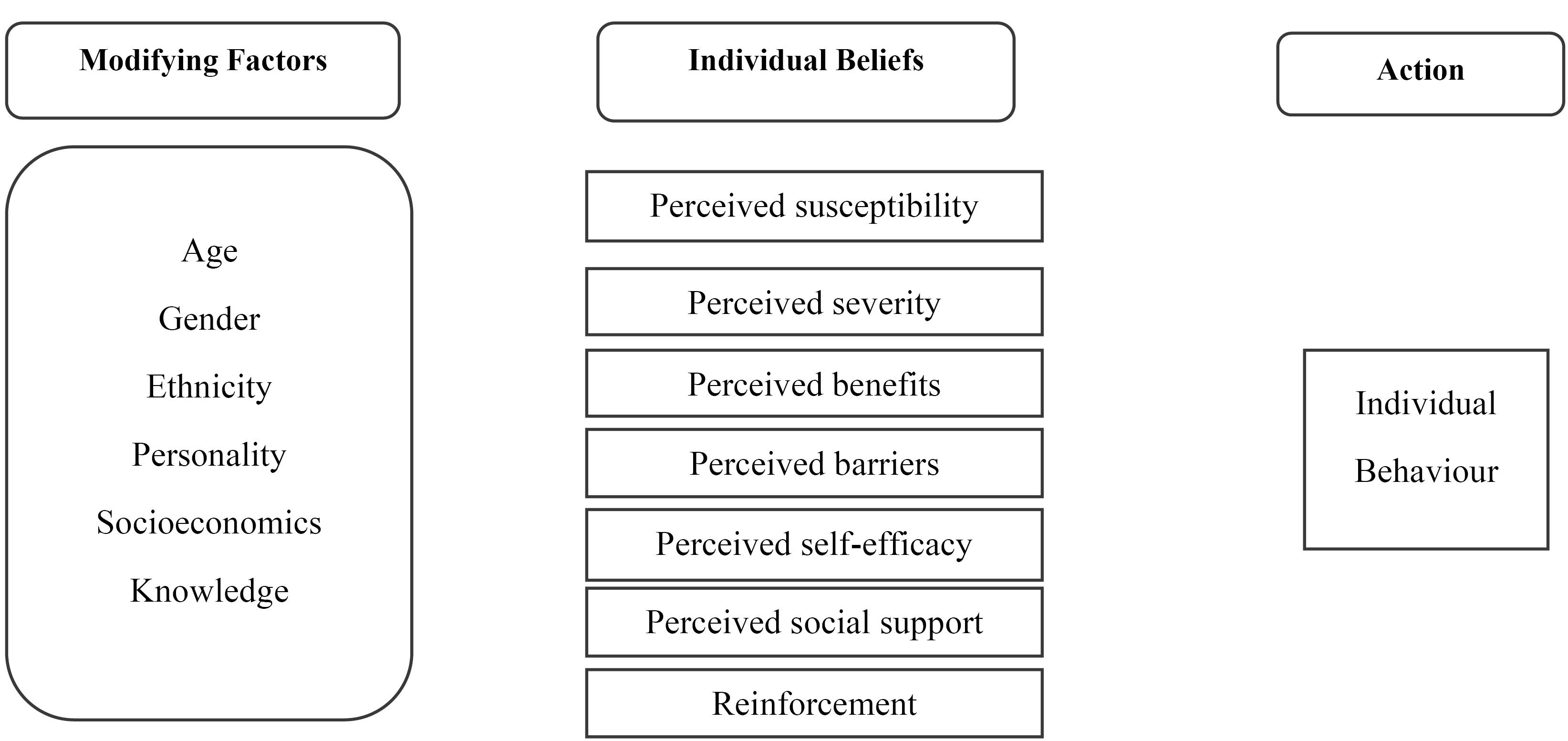
Figure 1.
The Integrated Health Belief Model as the Theoretical Framework of the Study
.
The Integrated Health Belief Model as the Theoretical Framework of the Study
Materials and Methods
Research Population and Design
The present study employed a theory-based, experimental two-arm design using a pretest-posttest approach with follow-up evaluation. The study was conducted on 138 female primary school students in Eslamshar, a city in Tehran province known for its relatively poor health indicators. Due to the socio-economic conditions of Eslamshahr county, including its proximity to Tehran, its suitability for housing internal and external migrants (mainly Afghan immigrants), and the relatively low standard of living, pediculosis has emerged as a significant public health concern. According to the latest statistics on pediculosis at the time of the study, among 32 314 examined female primary school students in urban areas of Eslamshahr county, 914 were diagnosed with pediculosis, showing the highest infection rate compared to middle and high school students (21).
The initial recruitment process involved a multistage cluster sampling method, where 51 primary schools were initially identified, from which two were randomly selected. Subsequently, one primary school was randomly assigned to the intervention group and the other to the control group. The methodology for selecting schools and students and the random allocation into intervention and control groups is illustrated in Figure 2. Students in the intervention group underwent the intervention, whereas those in the control group received no intervention.
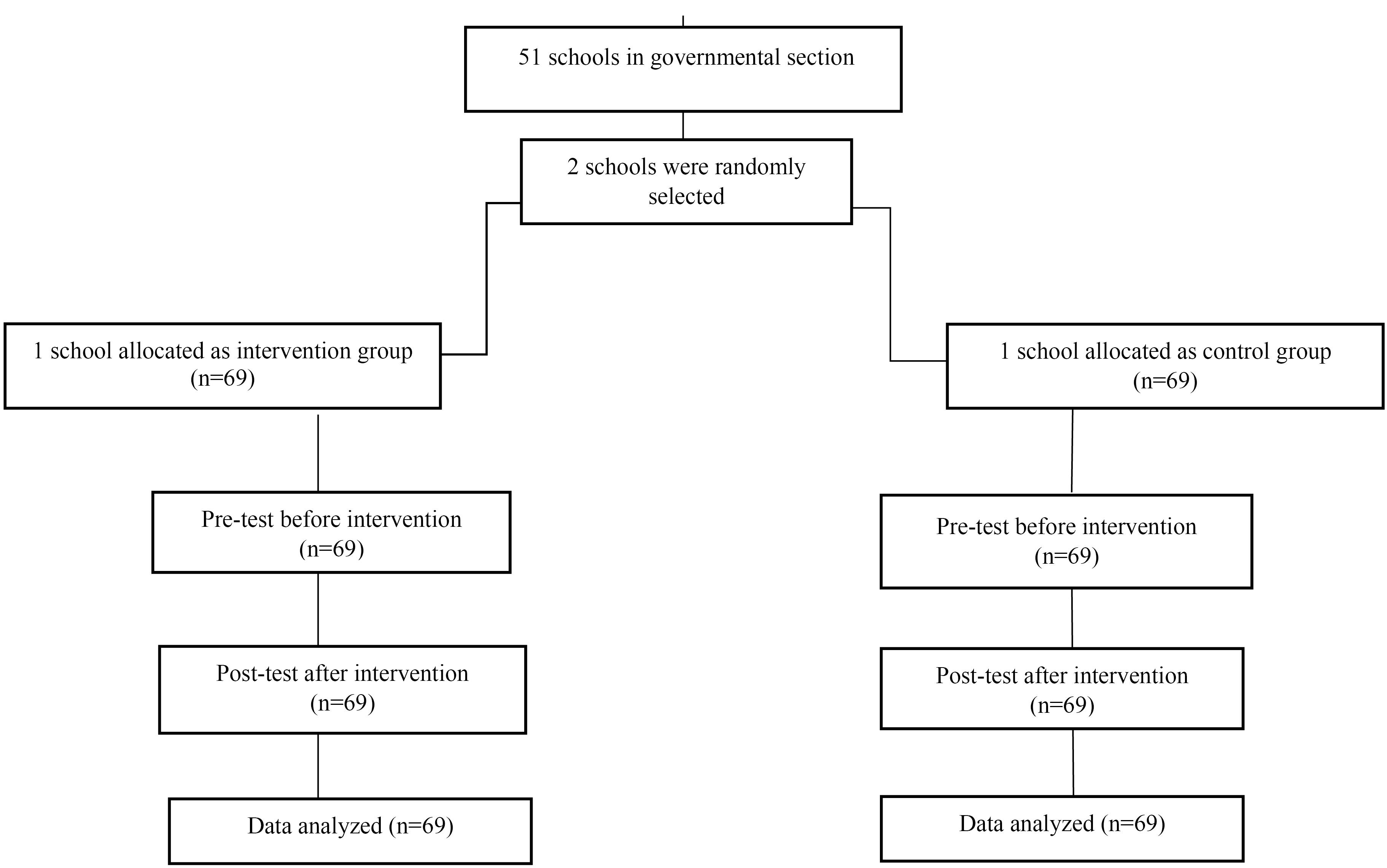
Figure 2.
CONSORT Diagram of the Study
.
CONSORT Diagram of the Study
The sample size was determined according to the results of a previous study (22), using the formula:
where (Z1- α½ = 1.96, Z1-β = 1.28)
Assuming an expected 10% attrition rate, the required sample size was calculated to be 69 students per group (α = 1.96, β = 1.28).
Before the intervention, both groups were evaluated for potential confounding variables, including age, parental education, parental employment, family size, and history of head lice infections. No significant differences were identified between the groups (P > 0.05), indicating their comparability for matching purposes.
Inclusion and Exclusion Criteria
The inclusion criteria included female students in grade 5 at primary schools in Eslamshar, absence of head lice infestation, willingness to participate, and provision of informed parental consent. Participants were excluded if they withdrew at any stage of the research or relocated during the study.
Measures
A questionnaire was developed based on IHBM constructs to evaluate participants’ knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, social support, self-efficacy, reinforcement, and preventive behaviors related to head lice infection. The questionnaire was developed using various sources, including literature reviews, peer-reviewed credible Iranian and international journals, and articles on head lice infestation. It also drew upon previously validated questionnaires from Persian and foreign studies, such as those by Moshki et al (23), Gholamnia Shirvani (17), and the national guidelines for head lice infestation (24). Additionally, discussions among the research team members contributed to the development of the questionnaire.
The questionnaire comprises 54 items covering various aspects of IHBM as follows: 13 items related to knowledge, 6 items measuring perceived susceptibility and perceived severity, 7 items related to perceived benefits, 9 items focusing on perceived barriers, 6 items assessing self-efficacy, 4 items addressing preventive behaviors, 5 items concerning social supports, and 4 items examining reinforcement (see Table 1).
Table 1.
Description of the Study Instrument
|
Construct
|
No. of Items (Format)
|
Scoring (Range)
|
Reliability Coefficient
|
| 1) Knowledge: Refers to theoretical or practical understanding of head lice infestation-related information. |
13 items (True-False-I don’t know) |
Correct response = 2, I don’t know response = 1, Incorrect response = 0
(0-26) |
ICC = 0.75 |
| 2) Perceived Susceptibility: Refers to the subjective assessment of the risk of developing head lice infestation. |
6 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(6-18) |
Cronbach’s Alpha = 0.75 |
| 3) Perceived Severity: Refers to one’s perception of the seriousness of head lice infestation and its potential consequences. |
6 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(6-18) |
Cronbach’s Alpha = 0.76 |
| 4) Perceived Benefits: Refers to perceived advantages from head lice infestation-related preventive behaviors |
7 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(7-21) |
Cronbach’s Alpha = 0.87 |
| 5) Perceived Barriers: Refers to perceived obstacles to adopting head lice infestation-related preventive behaviors. |
9 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(9-27) |
Cronbach’s Alpha = 0.75 |
| 6) Self-efficacy: Refers to an individual’s belief in their ability to perform head lice-related preventive behaviors successfully. |
6 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(6-18) |
Cronbach’s Alpha = 0.84 |
| 7) Preventive Behaviors: Refers to actions taken to prevent head lice infestation. |
4 items (4-point Likert scale) |
always = 1, sometimes = 2, seldom = 3, never = 4
(4-16) |
Cronbach’s Alpha = 0.75 |
| 8) Social Support: Refers to perceived support from others, particularly family and friends, for adopting preventive behaviors. |
5 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(5-15) |
Cronbach’s Alpha = 0.75 |
| 9) Reinforcement: Refers to responses from others that affect whether or not the behavior will be repeated. |
4 items (3-point Likert scale) |
agree = 1, no idea = 2, disagree = 3
(4-12) |
Cronbach’s Alpha = 0.75 |
Additionally, a separate questionnaire was used to collect demographic data from participants, including age, parental education level, family size, personal history of head lice infection, and family members’ history of head lice infestations.
Validity and Reliability Assessment
Face and content validity were evaluated to ensure the questionnaire’s accuracy and comprehensiveness. Reliability was assessed through test-retest analysis and by calculating internal consistency using Cronbach’s alpha coefficients.
Content and Face Validities
The evaluation of face validity involves ensuring that the test is understood and perceived in the same way by both the target group and the researchers. This includes verifying that the language and design of the instruments are appropriate and agreeable to the target group. The items must be clear, easily comprehensible, well-structured, and visually appealing to instill confidence and comfort in the target group while completing the questionnaire. Face validity was assessed through qualitative and quantitative methods, including feedback from experts and target group members.
Content validity was assessed using qualitative methods, such as expert committee review, and quantitative measures, including content validity ratio (CVR) and content validity index (CVI). The items were formatted into a content validity assessment tool for evaluation. In the qualitative phase, a panel of 10 experts specializing in health education and promotion, epidemiology, and psychology assessed the scale. They provided feedback on various aspects, including content, grammar, sentence length, word count, item order, potential additions, and cultural relevance. Based on their input, adjustments were made to the questionnaire. Subsequently, CVR and CVI were employed to validate the relevance and suitability of each item.
To this end, the experts received a questionnaire divided into two main sections. Following the Waltz and Basel method, the first section evaluated CVI using a 4-point Likert scale, rating each item’s pertinence, clarity, and simplicity. For instance, experts could rate items as “not relevant”, “somewhat relevant”, “quite relevant”, or “highly relevant”. The CVI for each item was determined by dividing the total number of experts who rated the item as 3 or 4 by the total number of experts involved in the evaluation. Items with a CVI exceeding 0.79 were deemed acceptable. To compute CVR, experts assessed the necessity of each item using a 3-point Likert scale, which included options such as “necessary”, “useful but not necessary”, or “not necessary”. According to Lawshe’s table, for a panel of 10 experts, an item was considered necessary if CVR exceeded 0.62.
Reliability
The reliability of the questionnaire sub-scales was assessed by analyzing internal consistency using Cronbach’s alpha coefficient. To evaluate the test-retest stability of the knowledge construct, 15 students who had initially completed the questionnaire were randomly selected and instructed to retake it after a 10-day interval.
Intervention
The study employed a pretest-posttest intervention design. In the pretest phase, both groups completed self-administered, paper-based questionnaires that assessed their knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, perceived self-efficacy, social support, and reinforcement related to head lice prevention. The educational approaches and frequency of educational sessions were tailored based on the students’ pretest scores. Following a comprehensive data analysis and evaluation of educational needs, decisions were made regarding the required number of sessions, critical topics, key content areas, and syllabi relevant to the training.
To ensure the readability, comprehensibility, and simplicity of the educational materials, a pilot test was conducted with a sample of 10 individuals who were not included in the primary study before the main research commenced. The educational content was developed based on the constructs of the IHBM and adapted from resources authorized by the Ministry of Health, including two pamphlets (for students and their parents) and a guide for health educators on head lice treatment and prevention. A total of 6 educational sessions were conducted for students, each lasting 35-45 minutes. These sessions were held in educational settings, specifically in classrooms and school meeting rooms. Lecture presentations, video screenings, question-and-answer segments, group discussions, and role-playing activities were employed during these sessions. The first session focused on increasing participants’ knowledge and perceived susceptibility to head lice infestation. The second session aimed to enhance participants’ understanding of the severity of infestation and the benefits of preventive behaviors through lectures and video demonstrations illustrating the consequences of pediculosis. The third session involved group discussions to identify and address perceived barriers to head lice prevention from the students’ perspective. The fourth session included role-playing activities and additional video demonstrations to promote self-efficacy in adopting preventive behaviors. Additionally, one session was dedicated to mothers who received lecture presentations and pamphlets to address the constructs of knowledge, social support, and reinforcement (see Supplementary file 1).
Data Analysis
The collected data were analyzed using SPSS version 16. To facilitate comparison, the scores of all variables were converted to a scale of 100. The Kolmogorov-Smirnov test showed that IHBM variables do not have a normal distribution. Therefore, non-parametric statistical tests were used for data analysis. The analysis involved two phases:
simple
-
1) Descriptive statistics: Frequencies, means, standard deviations, and chi-square (X2) tests were employed to describe the participants’ demographic characteristics and the baseline characteristics of the participants.
-
2) Inferential statistics: The Wilcoxon signed-rank test was used to compare mean scores for each IHBM construct across three time points (pre-test, immediate post-test, and two-month follow-up) within each group. Mann-Whitney U test was employed to compare differences in mean scores for each IHBM construct across the intervention and control groups at each time point.
Results
Demographic Characteristics
A total of 138 female primary school students participated in this study. Randomization was achieved between the two groups by controlling for relevant variables such as age, gender, education level, family size, parental employment status, personal history of head lice infection, and family history of head lice infection. The findings showed no significant difference between the intervention and control group for any of these variables (P < 0.05), as illustrated in Table 2.
Table 2.
Demographic Characteristics of Participants in Intervention and Control Groups
|
Variables
|
Control Group
|
Intervention Group
|
P
-value*
|
| Age |
11 years |
38 |
32 |
0.27 |
| 12 years |
31 |
38 |
| Father’s education |
Primary school |
12 |
18 |
0.75 |
| Diploma |
32 |
34 |
| Bachelor’s and higher |
20 |
18 |
| Mother’s education |
Illiterate |
16 |
22 |
0.45 |
| Primary school |
37 |
38 |
| Diploma |
14 |
10 |
| Father’s employment |
Laborer |
6 |
14 |
0.125 |
| Self-employed |
24 |
23 |
| Employee |
38 |
30 |
| Mother’s employment |
Employee |
18 |
18 |
0.96 |
| Housewife |
51 |
52 |
| Family size |
3 people |
10 |
10 |
0.91 |
| 4 people |
45 |
43 |
| 5 people and more |
14 |
16 |
| History of head lice infection |
Yes |
17 |
12 |
0.26 |
| No |
52 |
57 |
| Contamination of family members |
Yes |
4 |
2 |
0.39 |
| No |
65 |
68 |
Content and Face Validities for the Instrument
During the quantitative evaluation of face validity, all items achieved impact scores above 1.5 (ranging from 2.3 to 4.7) and were consequently retained in the final assessment tool. Expert feedback obtained during the qualitative content validity assessment phase was reviewed and incorporated. The Lawshe method was used to quantitatively assess the content validity of the tool, showing good content validity in this study. CVR ranged from 0.6 to 1.00, while CVI varied between 0.7 and 1.00.
Reliability of the Instrument
As seen in Table 1, all constructs had Cronbach’s alpha values above 0.70, suggesting strong internal consistency and reliability of the items. Additionally, the knowledge construct demonstrated an intra-class correlation coefficient (ICC) of 0.75, indicating satisfactory test-retest reliability.
Evaluation of Program Effectiveness
Evaluating the effectiveness of the educational intervention involved comparing changes in the IHBM constructs between the intervention and control groups. Data analysis revealed notable improvements in the intervention group in terms of knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, self-efficacy, and preventive behaviors (Table 3). However, no significant difference was observed in the reinforcement construct between the two groups.
Table 3.
Comparison of Intervention and Control Groups Regarding IHBM Constructs’ Scores Before and After the Intervention
|
Constructs
|
Groups
|
Before Intervention
|
Immediately After
|
P
Value*
|
2 Months After
|
P
Value**
|
|
(M±SD)
|
(M±SD)
|
|
(M±SD)
|
|
| Knowledge |
Intervention |
70.23 ± 8.28 |
86.28 ± 6.2 |
0.001 |
88.38 ± 6.58 |
0.001 |
| Control |
72.53 ± 7.86 |
73.06 ± 7.24 |
0.75 |
74.65 ± 7.58 |
0.03 |
|
P value |
|
0.001*** |
|
0.001**** |
|
| Perceived susceptibility |
Intervention |
56.76 ± 16.94 |
64.75 ± 14.19 |
0.002 |
70.71 ± 11.93 |
0.001 |
| Control |
63.52 ± 13.33 |
63.28 ± 14.24 |
0.55 |
60.14 ± 14.91 |
0.105 |
|
P value |
|
0.007 |
|
0.001 |
|
| Perceived severity |
Intervention |
51.18 ± 25.54 |
62.30 ± 24.01 |
0.001 |
62.58 ± 25.08 |
0.001 |
| Control |
54.70 ± 58.23 |
58.23 ± 23.89 |
0.75 |
61.83 ± 25.93 |
0.06 |
|
P value |
|
0.27 |
|
0.59 |
|
| Perceived benefits |
Intervention |
73.56 ± 16.14 |
84.99 ± 12.04 |
0.001 |
84.36 ± 16.76 |
0.038 |
| Control |
82.18 ± 14.73 |
85.60 ± 12.76 |
0.176 |
79.17 ± 13.36 |
0.26 |
|
P value |
|
0.011 |
|
0.42 |
|
| Perceived barriers |
Intervention |
25.15 ± 17.14 |
19.44 ± 13.95 |
0.001 |
16.18 ± 17.30 |
0.001 |
| Control |
19.78 ± 15.19 |
19.96 ± 13.28 |
0.176 |
19.90 ± 18.63 |
0.017 |
|
P value |
|
0.02 |
|
0.127 |
|
| Perceived self-efficacy |
Intervention |
64.16 ± 31.08 |
87.64 ± 21.95 |
0.001 |
91.78 ± 14.11 |
0.001 |
| Control |
80.95 ± 31.90 |
89.76 ± 20.60 |
0.08 |
83.68 ± 19.93 |
0.042 |
|
P value |
|
0.02 |
|
0.042 |
|
| Social support |
Intervention |
61.42 ± 22.73 |
72.28 ± 29.20 |
0.001 |
81.25 ± 25.65 |
0.001 |
| Control |
67.82 ± 23.56 |
68.98 ± 30.97 |
0.07 |
75.79 ± 27.62 |
0.08 |
|
P value |
|
0.13 |
|
0.02 |
|
| Reinforcement |
Intervention |
65.17 ± 24.16 |
70.89 ± 27.96 |
0.18 |
65.71 ± 27.55 |
0.4 |
| Control |
68.65 ± 21.71 |
68.47 ± 30.73 |
0.76 |
61.77 ± 34.42 |
0.27 |
|
P value |
|
0.17 |
|
0.25 |
|
| Preventive behaviors |
Intervention |
73.52 ± 9.65 |
78.79 ± 6.39 |
0.001 |
77.59 ± 8.29 |
0.001 |
| Control |
77.95 ± 6.65 |
79.22 ± 5.09 |
0.13 |
79.24 ± 5.62 |
0.03 |
|
P value |
|
0.01 |
|
0.04 |
|
Note. IHBM: Integrated health belief model; SD: Standard deviation.
* Wilcoxon test for after intra-group comparison (before vs. immediately after the intervention), with a significance level of 0.05; ** Wilcoxon test for intra-group comparison (before vs. 2 months after the intervention), with a significance level of 0.05; *** Mann-Whitney U test for between-groups comparison (before vs. immediately after the intervention), with a significance level of 0.05;**** Mann-Whitney U test for between-groups comparison (before vs. 2 months after the intervention, with a significance level of 0.05.
Discussion
This study focused on head lice, a prevalent issue among school-aged children. It aimed to investigate the impact of educational interventions rooted in the IHBM on promoting head lice prevention behaviors. The findings confirm the effectiveness of such interventions and provide valuable insights for designing pediculosis prevention strategies.
Previous studies in Iran have demonstrated that the frequency of pediculosis among female primary school students is six times greater than among male students (25). According to a systematic review, infection rates ranged from 1.25% to 56.15% in various studies focusing only on female students (26). After the intervention, a notable difference in preventive behavior scores was observed in the current study.
One important preventive behavior against head lice is regular bathing, which plays a critical role in preventing head lice infestation. Several studies have reported a significant relationship between head lice infestation and the availability of bathing facilities at home (27,28). Another study showed a significant relationship between using shared combs among students and head lice (29-31).
Maleki et al found a strong association between head lice infection and poor hygiene practices such as using shared personal items, inadequate handwashing, and infrequent changing of clothes (32). The results of this study are consistent with those of Nezhadali et al (33) and Moshki et al (23). Among the constructs of the HBM, perceived susceptibility emerged as one of the strongest predictors of preventive behavior in a previous study (34). This suggests that students are more likely to adopt preventive behaviors if they believe they are at risk of contracting head lice infection. The mental belief is that a person may suffer from a disease or a harmful state due to a particular behavior. In line with our study, Moshki et al reported increased perceived susceptibility among students following the intervention (23). Similarly, Motamedi and colleagues’ study on leishmaniasis among students demonstrated a post-intervention increase in perceived susceptibility (35), confirming that perceived susceptibility is one of the influential factors in adopting preventive behavior. Effective natural prevention depends largely on an individual’s accurate understanding of their vulnerability and the related health risks.
Another key construct of the theoretical framework of the present research was perceived severity, which refers to a person’s perception of the seriousness of a disease or its consequences. Our findings showed that educational intervention successfully increased the perceived severity of head-lice infection in the intervention group. However, the mean score of perceived severity did not significantly differ between the groups after the intervention. This finding is inconsistent with the results of previous studies, such as that of Moshki et al, who reported significantly higher post-intervention severity scores in the intervention group compared with the control group (23). A possible explanation for this discrepancy may be that students do not perceive head lice as a serious health threat. Notably, the severity variable acts as a double-edged sword; that is, when perceived as excessively high, it may lead to denial or failure to adopt preventive behaviors (36). Therefore, it is important to highlight the perceived severity of the symptoms of pediculosis in order to enhance individuals’ readiness to engage in preventive behaviors. Although perceived severity and sensitivity can create a force for behavior change, they cannot alone determine the individual’s actions. The likelihood of action also depends on individuals’ beliefs in the usefulness of behavior to reduce the risk of illness or to perceive the benefits of health action.
Another key finding of the present research was a significant change in the perceived benefits score in the experimental group immediately after the intervention, compared to the control group. Perceived benefits are a critical factor in encouraging individuals to adopt preventive health behaviors (37). These results align with Moshki and colleagues’ finding about preventive behaviors against head lice infestation (23) and Lotfi Mainbolagh and colleagues’ findings about eating habits in elementary school students (38).
One pivotal objective of this study was to compare the mean changes of perceived barriers to practicing preventive behaviors against head lice. Perceived barriers, often conceptualized as the obstacles or costs of adopting a new behavior, have been identified in some studies as the strongest predictors of preventive health behaviors (33). Our findings showed a significant decrease in the mean score of perceived barriers following the intervention in the experimental group. This finding is consistent with previous results reported by Moshki (23) and Jadgal et al (39).
Perceived self-efficacy, a person’s judgment of their ability to organize and perform a health-promoting behavior, plays a crucial role in overcoming obstacles to engaging in health behaviors. (40). It is also a key construct in the HBM and has been widely used in many intervention studies (41,42). People with a high perceived self-efficacy are more committed to challenging activities and tend to devote more time and effort to these activities. Moreover, they are more likely to contribute to maintaining and regaining healthy behaviors, even after a failure (43). This finding has also been reported by Nezhadali and Motamedi et al (33,35). Our study’s findings, which revealed a significant increase in students’ knowledge of head lice following the intervention, underscore the importance of education in preventing head lice infestations. This acknowledgment of education’s role in health promotion is a key takeaway from our research.
However, the findings were expected. Previous studies have reported low levels of knowledge about pediculosis among students (17,44-46), and educational interventions have increased the knowledge of preventing head lice in the intervention groups (17,23,47). Knowledge about symptoms, transmission routes, preventive behaviors, and treatment options can enhance awareness of this infection and help prevent head lice infestations in schoolchildren.
Perceived social support, which encompasses social relationships and interpersonal interactions, has been shown to benefit an individual’s health and well-being (48,49). In the present study, perceived social support refers to students’ perception of the support they receive from people around them, especially family members, in engaging in preventive behaviors. A survey by Ahmadi on the effect of peer education on students’ health-promoting behaviors indicated a significant increase in perceived social support after the intervention, which aligns with the results of our study (50).
In the present study, reinforcement refers to students’ perception of the encouragement, admiration, and rewards they receive from their family and relatives for engaging in preventative behaviors. Our findings revealed no significant difference between the intervention and control groups before and after the intervention. These results do not align with the findings of Soleiman Ekhtiari et al (51). This reinforcing process typically occurs when a person is encouraged (by themselves or others) to engage in health-promoting behaviors or otherwise punished for failing to do so (52). The limited time allocated to this construct within the educational intervention (only 10 minutes in a single session) may have been insufficient to produce a meaningful change. A more family-centered approach, involving additional sessions and diverse educational strategies (e.g., group discussions), is likely needed to enhance social support and empowerment in addition to those employed in the current study.
Ultimately, theory-based interventions, particularly those rooted in theory, should be considered crucial strategies for promoting preventive behaviors against pediculosis infestation among students by addressing both facilitating factors and enabling determinants.
Limitations
This study has some limitations. First, the use of self-report questionnaires to collect student responses may lead to social desirability bias, as students may provide responses they believe align with the research team’s expectations. The second constraint pertains to the sample size and composition, as only female students were included due to institutional restrictions, thereby excluding the male primary school student population. A third limitation concerns the participants’ socio-economic background, as the study did not explore how students’ social and economic status may have impacted the results.
Conclusion
Our study highlights the importance of implementing theory-based interventions that address facilitating factors and enabling determinants as a practical approach to promote preventive behaviors against pediculosis among students. Health specialists should be equipped with the knowledge and skills necessary to design and implement such interventions for at-risk students in school settings.
Overall, based on the findings of our study, the use of theoretical frameworks, particularly the IHBM, is recommended for the design, implementation, and evaluation of school-based interventions targeting pediculosis. Furthermore, it is suggested that future studies implement interventional programs in male students as well. When feasible, alternative and more objective evaluation methods should be employed alongside self-report questionnaires (e.g., family-reported data and observational methods). Moreover, it is recommended that future interventions place greater emphasis on students’ families.
Acknowledgments
The authors would like to thank all the students who participated in this study.
Competing Interests
The authors declare no conflict of interests in this study.
Data Availability Statement
The data from this study will be available upon request.
Ethical Approval
All participants were assured of the confidentiality of their data and provided written consent prior to participation. Participants had the freedom to withdraw from the study at any time. The study environment was conducive to providing accurate and reliable responses. Ethical approval for the study was obtained from the Ethics Committee of Shahid Beheshti University of Medical Sciences (Ethical Code: 6727). After the intervention, the control group was granted access to the same educational materials (slides) used by the experimental group.
Funding
The authors confirm that no financial support was received for the research presented in this article.
Supplementary Files
Supplementary file 1. Educational Content
(pdf)
References
- Khamaiseh AM. Head lice among governmental primary school students in southern Jordan: prevalence and risk factors. J Glob Infect Dis 2018; 10(1):11-5. doi: 10.4103/jgid.jgid_19_17 [Crossref] [ Google Scholar]
- Bekri G, Shaghaghi A. Prevalence of Pediculus humanus capitis and associated risk factors among elementary school-aged girls in Paveh, West Iran. J Infect Dev Ctries 2022; 16(9):1506-11. doi: 10.3855/jidc.11930 [Crossref] [ Google Scholar]
- Hatam-Nahavandi K, Ahmadpour E, Pashazadeh F, Dezhkam A, Zarean M, Rafiei-Sefiddashti R. Pediculosis capitis among school-age students worldwide as an emerging public health concern: a systematic review and meta-analysis of past five decades. Parasitol Res 2020; 119(10):3125-43. doi: 10.1007/s00436-020-06847-5 [Crossref] [ Google Scholar]
- Akbari M, Sheikhi S, Rafinejad J, Akbari MR, Pakzad I, Abdi F. Prevalence of pediculosis among primary school-aged students in Iran: an updated comprehensive systematic review and meta-analysis. J Med Entomol 2022; 59(6):1861-79. doi: 10.1093/jme/tjac117 [Crossref] [ Google Scholar]
- Nazari M, Goudarztalejerdi R, Anvari Payman M. Pediculosis capitis among primary and middle school children in Asadabad, Iran: an epidemiological study. Asian Pac J Trop Biomed 2016; 6(4):367-70. doi: 10.1016/j.apjtb.2016.03.002 [Crossref] [ Google Scholar]
- Sayyad S, Vahabi A, Vahabi B, Sayyadi M, Ahmadian M. Head louse (Pediculus humanus capitis) infestation in primary schoolchildren in rural areas of Paveh county, Kermanshah province. J Chem Pharm Sci. 2016(7):35-8.
- Moemenbellah-Fard MD, Nasiri Z, Azizi K, Fakoorziba MR. Head lice treatment with two interventions: pediculosis capitis profile in female schoolchildren of a rural setting in the south of Iran. Ann Trop Med Public Health 2016; 9(4):245-50. doi: 10.4103/1755-6783.184790 [Crossref] [ Google Scholar]
- Alborzi M, Shekarriz-Foumani R. The prevalence of Pediculus capitis among primary schools of Shahriar county, Tehran province, Iran, 2014. Nov Biomed 2016; 4(1):24-7. doi: 10.22037/nbm.v4i1.9416 [Crossref] [ Google Scholar]
- Toloza A, Vassena C, Gallardo A, González-Audino P, Picollo MI. Epidemiology of pediculosis capitis in elementary schools of Buenos Aires, Argentina. Parasitol Res 2009; 104(6):1295-8. doi: 10.1007/s00436-008-1324-6 [Crossref] [ Google Scholar]
- Ismail MT, Kabakibi MM, Al-Kafri A. Epidemiology of pediculosis capitis among schoolchildren in Damascus, Syria. Indian J Paediatr Dermatol 2018; 19(4):331-4. doi: 10.4103/ijpd.IJPD_123_17 [Crossref] [ Google Scholar]
- Ruankham W, Winyangkul P, Bunchu N. Prevalence and factors of head lice infestation among primary school students in Northern Thailand. Asian Pac J Trop Dis 2016; 6(10):778-82. doi: 10.1016/s2222-1808(16)61129-5 [Crossref] [ Google Scholar]
- Eroglu F, Basaran Ü, Kürklü CG, Yüceer M, Yalcıntürk RG, Tanrıverdi M. Pediculosis capitis is a growing neglected infestation due to migration in southeast Turkey. Parasitol Res 2016; 115(6):2397-401. doi: 10.1007/s00436-016-4990-9 [Crossref] [ Google Scholar]
- Nazari M, Goudarztalejerdi R, Moradi A. Investigation of pediculosis prevalence and associated factors in the central prison of Hamadan in 2013. Pajouhan Sci J 2015;13(2):13-20. [Persian].
- Kassiri H, Mehraghaei M. Assessment of the prevalence of pediculosis capitis and related effective features among primary schoolchildren in Ahvaz county, southwest of Iran. Environ Sci Pollut Res Int 2021; 28(18):22577-87. doi: 10.1007/s11356-020-12284-9 [Crossref] [ Google Scholar]
- Ghaffari M, Nasiri Esfahani S, Rakhshanderou S, Hosseini Koukamari P. Evaluation of health belief model-based intervention on breast cancer screening behaviors among health volunteers. J Cancer Educ 2019; 34(5):904-12. doi: 10.1007/s13187-018-1394-9 [Crossref] [ Google Scholar]
- Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. John Wiley & Sons; 2008.
- Gholamnia Shirvani Z, Amin Shokravi F, Ardestani MS. Effect of designed health education program on knowledge, attitude, practice and the rate pediculosis capitis in female primary school students in Chabahar city. J Shahrekord Univ Med Sci 2011;13(3):25-35. [Persian].
- Warren-Findlow J, Prohaska TR. Families, social support, and self-care among older African-American women with chronic illness. Am J Health Promot 2008; 22(5):342-9. doi: 10.4278/ajhp.22.5.342 [Crossref] [ Google Scholar]
- Peterson JA, Yates BC, Hertzog M. Heart and soul physical activity program: social support outcomes. Am J Health Behav 2008; 32(5):525-37. doi: 10.5555/ajhb.2008.32.5.525 [Crossref] [ Google Scholar]
- Green LW, Kreuter MW. Health Program Planning: An Educational and Ecological Approach. New York: McGraw-Hill; 2005.
- Kolivand A. Effect of Educational Intervention on Preventive Behaviors of Head Lice Infestation among Primary School Girls in Eslamshahr City, 2015–2016 [MSc thesis]. Tehran: Shahid Beheshti University of Medical Sciences, School of Public Health; 2016.
- Alizadeh Siuki H, Keshavarz M, Jafari A, Ramezani H. Effects of nutritional education on knowledge and behaviors of primary students in Torbat Heydariyeh. J Torbat Heydariyeh Univ Med Sci 2013;1(1):44-51. [Persian].
- Moshki M, Zamani-Alavijeh F, Mojadam M. Efficacy of peer education for adopting preventive behaviors against head lice infestation in female elementary school students: a randomised controlled trial. PLoS One 2017; 12(1):e0169361. doi: 10.1371/journal.pone.0169361 [Crossref] [ Google Scholar]
- Center for Infectious Disease Management. Educational Guide and National Guidelines for Care Pediculosis. 2016. Availble from: https://rey.tums.ac.ir/uploads/86/2022/May/29/%D9%BE%D8%AF%DB%8C%DA%A9%D9%84%D9%88%D8%B2%20%D8%AF%D8%B3%D8%AA%D9%88%D8%B1%D8%A7%D9%84%D8%B9%D9%85%D9%84%2095_1.pdf.
- Khosravani M, Ali Amiri S, Rafatpanah A, Bandak C, Latifi R, Moradi M, Mohemmi N, Abdollahi Harat F, Mohebbi Nodez SM, Hatami Z. A Review of Pediculosis Studies in Iran During Three Decades (1990–2020). J Health Sci Surveillance Sys 2021; 9(4):218-225. [ Google Scholar]
- Khosravani M, Amiri SA, Rafatpanah A, Bandak C, Latifi R, Moradi M. A review of pediculosis studies in Iran during three decades (1990-2020). J Health Sci Surveill Syst 2021; 9(4):218-25. doi: 10.30476/jhsss.2021.90450.1192 [Crossref] [ Google Scholar]
- Buczek A, Markowska-Gosik D, Widomska D, Kawa IM. Pediculosis capitis among schoolchildren in urban and rural areas of eastern Poland. Eur J Epidemiol 2004; 19(5):491-5. doi: 10.1023/b:ejep.0000027347.76908.61 [Crossref] [ Google Scholar]
- Rafie A, Kasiri H, Mohammadi Z, Haghighizade M. Pediculosis capitis and its associated factors in girl primary school children in Ahvaz city in 2005-2006. Iran J Infect Dis Trop Med 2009;45:41-5. [Persian].
- Albashtawy M, Hasna F. Pediculosis capitis among primary-school children in Mafraq governorate, Jordan. East Mediterr Health J 2012; 18(1):43-8. doi: 10.26719/2012.18.1.43 [Crossref] [ Google Scholar]
- Saddozai S, Kakarsulemankhel JK. Infestation of head lice, Pediculus humanus capitis, in school children at Quetta city and its suburban areas, Pakistan. Pak J Zool 2008; 40(1):45-52. [ Google Scholar]
- Al-Megrin WA. Assessment of the prevalence of pediculosis capitis among primary school girls in Riyadh, Saudi Arabia. Res J Environ Sci 2015; 9(4):193-99. doi: 10.3923/rjes.2015.193.199 [Crossref] [ Google Scholar]
- Maleky A, Yazdani-Charati J, Abdollahi F. The prevalence of pediculosis capitis and its associated risk factors in primary school students in Kalaleh, Iran in 2015. J Health Res Commun 2016;2(3):23-31. [Persian].
- Nezhadali A, Babazadeh T, Nadrian H, Allahverdipour H. Cognitive factors associated to pediculosis preventive behaviors among mothers of school-age children in Chaldoran county, Iran. J Multidiscip Healthc 2020; 13:19-26. doi: 10.2147/jmdh.S237101 [Crossref] [ Google Scholar]
- Carmel S. The health belief model in the research of AIDS-related preventive behavior. Public Health Rev 1990; 18(1):73-85. [ Google Scholar]
- Motamedi N, Hejazi SH, Hazavehei SM, Zamani AR, Saberi S, Rahimi E. Effect of education based on health belief model on promoting preventive behavior of coetaneous leishmaniasis. J Mil Med 2022;11(4):231-6. [Persian].
- Sharma M. Theoretical foundations of health education & health promotion. 3rd ed. Burlington, MA: Jones & Bartlett Learning; 2016.
- Taghdisi MH, Nejadsadeghi E. The effect of health education based on health belief model on behavioral promotion of urinary infection prevention in pregnant women. Journal of Research and Health 2012;2(1):44-54. [Persian].
- Lotfi Mainbolagh B, Rakhshani F, Zareban I, Alizadeh Sivaki H, Parvizi Z. The effect of peer education based on health belief model on nutrition behaviors in primary school boys. Journal of Research and Health 2012;2(2):214-26. [Persian].
- Jadgal KM, Zareban I, Rakhshani F, Alizadeh Siuki H, Lotfi Mayen Boulagh B, Hajilou E. The impact of health education based on health belief model on preventive behavior of unwanted pregnancy among Chabahar women. Journal of Health 2014;5(3):191-202. [Persian].
- Shojaeizadeh D, Heydarnia A, Ghofranipour F, Pakpour Hajiagha A, Saffari M. Health Education and Promotion Theories, Models and Methods. Tehran, Iran: Asar Sobhan Publications; 2012. [Persian].
- Schwarzer R, Antoniuk A, Gholami M. A brief intervention changing oral self-care, self-efficacy, and self-monitoring. Br J Health Psychol 2015; 20(1):56-67. doi: 10.1111/bjhp.12091 [Crossref] [ Google Scholar]
- Otsuka K, Taguri M, Dennis CL, Wakutani K, Awano M, Yamaguchi T. Effectiveness of a breastfeeding self-efficacy intervention: do hospital practices make a difference?0. 0Matern Child Health J 2014; 18(1):296-306. doi: 10.1007/s10995-013-1265-2 [Crossref] [ Google Scholar]
- Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol 2001; 52:1-26. doi: 10.1146/annurev.psych.52.1.1 [Crossref] [ Google Scholar]
- Zareban E, Abbaszade Bezi M, Movadi M, Mehrjoofard H, Ghafari HR. Evaluation of health education program for reducing head lice infestation among primary school girls. J Birjand Univ Med Sci 2006;13(1):25-31. [Persian].
- Heukelbach J, Ugbomoiko US. Knowledge, attitudes and practices regarding head lice infestations in rural Nigeria. J Infect Dev Ctries 2011; 5(9):652-7. doi: 10.3855/jidc.1746 [Crossref] [ Google Scholar]
- Magalhães P, Figueiredo EV, Capingana DP. Head lice among primary school children in Viana, Angola: prevalence and relevant teachers’ knowledge. Hum Parasit Dis 2011; 3:11-8. doi: 10.4137/hpd.s6970 [Crossref] [ Google Scholar]
- Bachok N, Nordin RB, Awang CW, Ibrahim NA, Naing L. Prevalence and associated factors of head lice infestation among primary schoolchildren in Kelantan, Malaysia. Southeast Asian J Trop Med Public Health 2006; 37(3):536-43. [ Google Scholar]
- Berkman LF. The relationship of social networks and social support to morbidity and mortality. In: Cohen S, Syme SL, eds. Social Support and Health. Academic Press; 1985. p. 241-62.
- Berkman LF, Glass T. Social integration, social networks, social support, and health. Soc Epidemiol 2000; 1(6):137-73. [ Google Scholar]
- Ahmadizadeh Fini E, Madani A, Alizadeh A, Ghanbarnejad A, Aghamolaei T. Effect of peer education on health promoting behaviors of junior high school students. Iran J Health Educ Health Promot 2015;3(2):105-15. [Persian].
- Soleiman Ekhtiari Y, Shojaeizadeh D, Rahimi Foroushani A, Ghofranipour F, Ahmadi B. The effect of an intervention based on the PRECEDE- PROCEED model on preventive behaviors of domestic violence among Iranian high school girls. Iran Red Crescent Med J 2013; 15(1):21-8. doi: 10.5812/ircmj.3517 [Crossref] [ Google Scholar]
- Michie S, West R, Campbell R, Brown J, Gainforth H. ABC of Behaviour Change Theories. London: Silverback Publishing; 2014.