J Educ Community Health. 12(1):60-67.
doi: 10.34172/jech.3257
Original Article
Comparing the Impacts of Gain Versus Loss Frame Messages on Complementary Feeding Behaviors of Mothers With Under Six-Month Infants: The Application of an Extended Parallel Process Model
Mohadeseh Mosalanezhad Data curation, Formal analysis, Software, Writing – original draft, 1
Leila Ghahremani Investigation, Methodology, Resources, Validation, Visualization, 2 
Mahin Nazari Investigation, Methodology, Resources, Supervision, Validation, Visualization, 2
Fatemeh Sadat Hosseini Data curation, Writing – original draft, Writing – review & editing, 3
Masoud Karimi Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – review & editing, 4, *
Author information:
1Student Research Committee, Department of Health Promotion, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran
2Research Center for Health Sciences, Institute of Health, Department of Health Promotion, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran
3Department of Health Promotion, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran
4Research Center for Health Sciences, Institute of Health, Department of Health Promotion, School of Health, Shiraz University of Medical Sciences, Al-Zahra Street, Shiraz, Iran
Abstract
Background: Timely initiation of appropriate complementary feeding (CF) plays an important role in the growth and development of infants. The aim of this study was to investigate the effect of two types of educational messages (gain and loss frames) on mothers’ knowledge, attitudes, and behavior regarding infant CF using the extended parallel process model.
Methods: This quasi-experimental study with intervention and control groups involved 90 mothers with 2-4-month-old infants selected by a multistage random sampling method. They were randomly assigned to one of the three intervention groups (gain frame, loss frame, and both messages) and a control group. The data collection instruments were a form with demographic information and a researcher-made questionnaire. Educational messages in the form of video clips (up to 4 minutes), text messages, and pictures were sent to the intervention groups via WhatsApp Messenger. A post-test was conducted one month after the intervention.
Results: After the intervention, significant differences were found in the mean scores for knowledge (P<0.001) and self-efficacy (P<0.001) between the intervention groups and the control group. A significant increase in mean scores for knowledge, perceived susceptibility, and self-efficacy was observed in all intervention groups. There were no significant differences between the three intervention groups in terms of changes in the mean values of the study variables.
Conclusion: The educational interventions had a moderate effect. The type of message did not influence the effectiveness of the intervention. Future studies should examine long-term effects and alternative message strategies. Health policymakers should consider integrating similar educational interventions into maternal health programs to improve maternal knowledge and self-efficacy.
Keywords: Infant, Complementary feeding, Behavior, Text messaging, Intervention
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Mosalanezhad M, Ghahremani L, Nazari M, Hosseini FS, Karimi M. Comparing the impacts of gain versus loss frame messages on complementary feeding behaviors of mothers with under six-month infants: the application of an extended parallel process model. J Educ Community Health. 2025; 12(1):60-67. doi:10.34172/jech.3257
Introduction
Nutrition is crucial for the growth and development of children (1,2). Breast milk is the optimal first feeding for infants (3), but from six months onwards, complementary foods are necessary to meet nutritional requirements (4). At this stage, the child is physiologically and neuromuscularly mature enough to eat semi-solid and solid foods (5-7). The World Health Organization (6) and the American Academy of Pediatrics (4) recommend exclusive breastfeeding for the first six months and the introduction of complementary feeding (CF) together with breast milk thereafter (8,9).
Timely and appropriate introduction of CF is essential for the health and development of infants (10). Introducing CF too early can lead to reduced breast milk intake, diarrhea, allergies, growth retardation (11), and immune and kidney disorders (12,13). Conversely, delayed CF can lead to physical and cognitive growth retardation (14-16). Poor-quality complementary foods can lead to malnutrition, stunted growth, and an increased risk of infant mortality (7,17,18).
Despite these risks, studies suggest that many mothers introduce complementary foods too early because they believe that breast milk alone is insufficient (4,19). Research in Indonesia found that less than 25% of infants aged 6–23 months received an age-appropriate diet (20). In Iran, Behzadifar et al reported a 47% rate of early introduction of CF (21), while Zarshanas et al observed that only 1% of mothers exclusively breastfed for 26 weeks, with 28% taking additional fluids (22).
The results underline the need for educational measures to encourage mothers to start CF for infants under six months of age in a timely and appropriate manner. There is evidence that the use of behavior change models increases the effectiveness of health education programs (23). Although fear appeals are traditionally used, their effectiveness was questioned by Ruiter et al in a review of 60 years of studies (24).
Since the 1950s, various theories have explained the cognitive processing and acceptance of fear appeals, with the extended parallel process model (EPPM) being one of the most important developments (25), which is depicted in Figure 1. The EPPM states that responses to health messages depend on the balance between perceived threat (risk susceptibility and severity) and perceived efficacy (self-efficacy and response efficacy). A low perceived threat leads to no response, whereas a high perceived threat with high efficacy results in danger control (adoption of recommendations). In addition, low efficacy triggers fear control (defensive reactions such as avoidance and denial) (26-30).
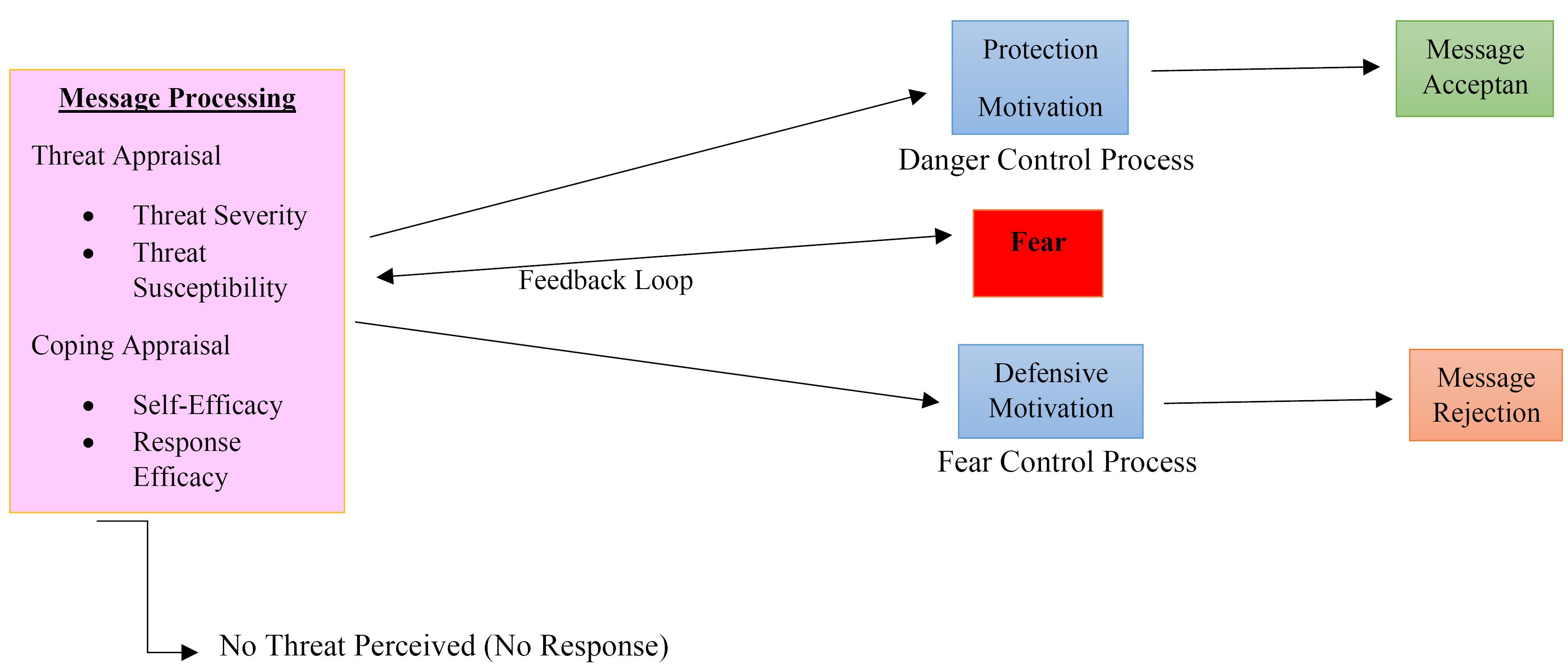
Figure 1.
The Extended Parallel Processing Model
Source. Witte (1992) (25)
.
The Extended Parallel Processing Model
Source. Witte (1992) (25)
Message framing plays a crucial role in health education interventions (25). Messages that highlight the risks of unhealthy behaviors are frequently used but often trigger fear-control responses (24). Research suggests that their effectiveness varies by behavior type; messages with losses influence risky behaviors such as smoking, while messages with gains that emphasize the benefits are more effective for behaviors such as healthy eating (31-32).
Despite extensive research on CF, there is limited evidence on the effectiveness of different message strategies in influencing mothers’ knowledge, attitudes, and behaviors related to timely and appropriate CF. While the EPPM is widely used in health education, its application to CF remains under-researched. In addition, previous studies have reported contradictory results on the effects of gain/loss messages, especially in behavioral contexts with different levels of risk. Given the critical role that proper CF plays in infant health and development and the potential that message framing has for improving behavior change interventions, this study aims to address this gap by examining how gain-framed and loss-framed messages influence mothers’ decision-making using the EPPM.
Materials and Methods
Study Design and Participants
All mothers with infants aged 2-4 months were included in this quasi-experimental study, which comprised an intervention group and a control group. The selection of mothers with infants aged 2–4 months was based on the critical developmental stage at which CF begins. At this age, the transition from exclusive breastfeeding to the introduction of solid foods takes place, making this an important period for education on appropriate feeding practices. Targeting mothers during this period can help identify potential feeding issues early and influence knowledge, attitudes, and behaviors related to CF before poor practices become established. The study was conducted in the comprehensive urban health centers of Jahrom in Fars province, Iran. Based on the study by Rafiyan et al (33), using NCSS-PASS-15 software and considering an alpha value of 0.05, a test power of 85%, a mean difference of 2.39, a design effect of 1.3, and an attrition rate of 10%, the sufficient sample size for each group in the study was calculated to be 25 people.
Participants were selected by a multistage randomization procedure. To this end, 4 centers were first randomly selected from the 8 comprehensive health centers in Jahrom, and each center was randomly assigned to one of the three intervention groups (receiving messages of the gain frame, the loss frame, and both messages) and a control group. Then, in each center, 25 women with infants aged 2–4 months who came to the center for routine healthcare were selected using simple randomization and, if they were satisfied and met the inclusion criteria, they were invited to participate in the study.
Inclusion Criteria for Infants
Two-to-four-month-old infants who were full-term (gestational age 37–42 weeks) and exclusively breastfed during participation in the study and did not suffer from a specific disease requiring early initiation of CF.
Inclusion Criteria for the Mothers
Those who were at least able to read and write, had a smart cell phone, were familiar with the messenger WhatsApp or similar messengers, and were willing to participate in the study.
Exclusion Criteria
They included death of the mother or the child or migration of the family, serious illness of the child during the study requiring hospitalization, non-compliance and regular participation in educational programs, and withdrawal from further participation in the study.
Instruments for Data Collection
The first part was a form with demographic information that included the child’s gender and date of birth, mother’s age, educational level, occupational status, and economic status of the family. The second part contained a multiple-choice knowledge questionnaire (7 questions) created by the researcher, where correct, incorrect, and I do not know answers were scored as 1, 0, and 0, respectively (e.g., What is the first sign of a child’s developmental disorder?).
The third part encompassed a questionnaire designed by the researcher based on the constructs of the EPPM. Five constructs were measured in this questionnaire, including perceived sensitivity, perceived severity, perceived self-efficacy, response efficacy, and intention. Perceived sensitivity included 9 items about the possibility of the child suffering from complications if starting CF too early or too late and about inappropriate infant feeding (e.g., if I start several different foods together, it will make my baby sick). Perceived severity consisted of 11 items on the extent of complications and risks of starting CF early or late and inappropriate feeding for infants (e.g., complications of early initiation of CF can cause health problems for my child in the future). In addition, perceived self-efficacy contained 9 items on the mother’s perceived ability to feed the baby CF in the right way and at the right time (e.g., despite being very busy, I can allocate enough time to prepare complementary food for my child). Response efficacy encompassed 12 items on the effectiveness of appropriate CF on the child’s health, growth, and development (e.g., initiating complementary food at the recommended age prevents disease in childhood). Finally, intention included 13 items on the intention to give CF at the right time and in the right way (e.g., I intend to exclusively breastfeed my child until he/she is 6 months old). All constructs were measured using a five-point Likert-type scale. After the intervention, instead of intention, behavior was assessed using a 4-item questionnaire that assessed the age at which the mothers started CF and the type of food they gave to their children.
The surface and content validity of the questionnaire were reviewed and confirmed by a panel of 8 health education and health promotion professionals (content validity rate > 0.75, content validity index > 0.8). The internal consistency of the questionnaire was checked by a pilot study with 14 people who had the same conditions as the participants in the study. The Cronbach’s alpha coefficient was calculated for five constructs between 0.6 and 0.85. External reliability was also measured by a test-retest at two-week intervals on a sample of 14 mothers, and the intraclass correlation coefficient was computed between 0.85 and 0.95.
Intervention
After the mothers had been selected to participate in the study, the aims of the study were explained to them, and they were assured that their information would remain confidential. They then signed the consent form and completed the questionnaire for the pre-test in a personal interview at the health center. Next, a virtual group was formed on WhatsApp for each of the three intervention groups and the control group. Based on the Iranian Ministry of Health guidelines on CF (34), educational messages were designed in the form of educational video clips (up to 4 minutes), text messages, and pictures in two forms of gain and loss frames. Six educational video clips were sent to each of the groups that received a gain and a loss message, and 8 educational video clips were sent to the group that received both types of messages over one month. The loss messages were about the negative health effects of early or late initiation or inappropriate CF on the infant’s health, growth, and development. In contrast, the ‘gain’ messages focused on the benefits of starting CF early and appropriately for the infant’s health, growth, and development.
The mothers’ questions were answered in the virtual groups by the main researcher so that there was appropriate interaction with the participants throughout the study. The control group received only routine educational and healthcare interventions during the study period. One month after the end of the educational intervention, a post-test was conducted for each group and the control group by completing the same questionnaires that were used before the intervention (Table 1).
Table 1.
Summary Table of the Intervention, Including Educational Objectives, Teaching Methods, and Other Important Details
|
Details
|
Component
|
| Target audience |
Mothers of infants under six months of age |
| Study groups |
- Loss-framed message group
- Mixed (gain + loss) message group
- Control group (routine education) |
| Educational objectives |
- Improving knowledge about complementary feeding
- Promoting a positive attitude toward the timely and appropriate introduction of complementary feeding
- Encouraging appropriate complementary feeding behavior |
| Teaching methods |
- Educational video clips (maximum of 4 minutes)
- Text messages
- Images |
| Message framing |
- Gain-framed messages: Benefits of timely and appropriate complementary feeding
- Loss-framed messages: Adverse health effects of early/late or inappropriate complementary feeding |
| Duration of the intervention |
One month |
| Type of implementation |
Virtual WhatsApp groups |
| Interaction |
Mothers’ questions answered by the main researcher in the group chat |
| Evaluation instruments |
Pre-test and post-test using questionnaires |
| The control group |
Received only routine health education and care |
Statistical Analysis
The data were processed and analyzed using SPSS software, version 25. The distributions of the demographic variables were compared between the intervention and control groups using the Chi-square test. As the data followed a normal distribution in the Kolmogorov-Smirnov test (P > 0.05), a one-way analysis of variance was used to compare the means between the intervention and control groups, and the paired t-test was also utilized for within-group comparisons. The analysis was interpreted at the 0.05 significance level.
Results
A total of 90 mothers completed the study. The demographic characteristics of the participants are summarized in Table 2. No significant differences were found between the four study groups in terms of mother’s age, infant’s age, infant’s gender, mother’s education level, mother’s employment status, or family economic status, indicating that the groups were comparable at baseline.
Table 2.
Frequency Distribution of Demographic Variables of Participants in the Study
|
Variable
|
|
Group*
|
P
-value
|
|
Intervention 1
|
Intervention 2
|
Intervention 3
|
Control
|
| Infant’s age in months (mean ± SD) |
|
3.99 (0.86) |
4.01 (0.69) |
4.1 (0.68) |
3.97 (1.04) |
0.16** |
| Mother’s age in years (mean ± SD) |
|
29.45 (5.16) |
30.47 (5.05) |
33.31 (4.7) |
33.18 (5.18) |
0.58** |
Infant’s gender
N (%) |
Male |
8 (33.3) |
10 (47.6) |
13 (56.5) |
10 (45.5) |
0.45*** |
| Female |
16 (66.7) |
11 (52.4) |
10 (43.5) |
12 (54.5) |
Mother’s education level
N (%) |
Elementary |
2 (8.3) |
1 (4.8) |
0 (0.0) |
0 (0.0) |
0.09*** |
| Secondary |
10 (41.7) |
4 (19.0) |
5 (21.7) |
6 (27.3) |
| College |
12 (50.0) |
16 (76.2) |
18 (78.3) |
16 (72.7) |
Mother’s job
N (%) |
Working at home |
0 (0.0) |
0 (0.0) |
2 (8.7) |
2 (9.1) |
0.07*** |
| Employed |
1 (4.2) |
5 (23.8) |
6 (26.1) |
8 (36.4) |
| Housewife |
23 (95.8) |
16 (76.2) |
15 (65.2) |
12 (54.5) |
Family’s economic status
N (%) |
Poor |
6 (25.0) |
7 (33.3) |
1 (4.3) |
2 (9.1) |
0.09*** |
| Moderate |
18 (75.0) |
13 (61.9) |
22 (95.7) |
19 (86.4) |
| Good |
0 (0.0) |
1 (4.8) |
0 (0.0) |
1 (4.5) |
Note. SD: Standard deviation; ANOVA: Analysis of variance. *Intervention 1: Gain frame messages; Intervention 2: Loss frame messages; Intervention 3: Both messages. ****One-way ANOVA; ***Chi-square test.
In terms of primary outcomes, no significant differences were observed between the intervention and control groups in the mean scores of the EPPM constructs before the intervention. After the intervention, however, there were significant differences between the intervention and control groups in the mean scores for knowledge (P < 0.001) and self-efficacy (P < 0.001). In particular, all three intervention groups (gain frame, loss frame, and both frames) showed significant increases in these constructs compared to the control group. The Bonferroni post-hoc test demonstrated that there were no significant differences between the three intervention groups in terms of knowledge and self-efficacy.
In within-group comparisons, the control group represented no significant changes in the mean scores of the EPPM constructs after the intervention. In contrast, significant increases in mean scores for knowledge, perceived susceptibility, and self-efficacy were observed in all three intervention groups. However, no significant differences in perceived severity and response efficacy scores were found in any of the groups after the intervention. In addition, no significant changes in behavior were noted in either the intervention or control group (Table 3).
Table 3.
Comparing Mean (SD) Scores of EPPM Constructs Before and After the Intervention Between and Within Study Groups
|
Construct
|
Time
|
Group*
|
P
-value**
|
|
Intervention 1
|
Intervention 2
|
Intervention 3
|
Control
|
| knowledge |
Before |
4.91 (0.51) |
5.81 (1.21) |
5.65 (0.48) |
5.18 (1.50) |
0.07 |
| After |
6.41 (0.53) |
4.47 (0.67) |
6.39 (0.72) |
5.45 (1.01) |
< 0.001 |
|
P-value*** |
|
< 0.001 |
0.03 |
< 0.001 |
0.24 |
|
| Perceived susceptibility |
Before |
36.45 (6.91) |
33.47 (7.98) |
34.95 (5.42) |
35.13 (6.04) |
0.49 |
| After |
38.37 (5.97) |
36.47 (7.39) |
38.04 (5.76) |
36.77 (7.54) |
0.72 |
|
P-value*** |
|
0.02 |
0.01 |
0.003 |
0.14 |
|
| Perceived severity |
Before |
50.12 (5.40) |
48.47 (6.22) |
49.65 (5.64) |
48.93 (4.69) |
0.75 |
| After |
50.79 (3.71) |
49.04 (5.67) |
51.26 (4.27) |
48.59 (5.89) |
0.21 |
|
P-value*** |
|
0.49 |
0.44 |
0.07 |
0.69 |
|
| Self-efficacy |
Before |
41.49 (4.24) |
42.14 (3.83) |
43.60 (2.03) |
41.90 (3.13) |
0.28 |
| After |
44.16 (1.01) |
44.33 (1.85) |
44.72 (0.54) |
42.13 (3.61) |
< 0.001 |
|
P-value*** |
|
0.02 |
0.02 |
0.01 |
0.75 |
|
| Response efficacy |
Before |
55.66 (5.79) |
55.52 (4.33) |
55.82 (5.49) |
54.81 (5.97) |
0.93 |
| After |
56.25 (4.48) |
56.04 (4.81) |
56.30 (4.48) |
54.59 (6.52) |
0.64 |
|
P-value*** |
|
0.51 |
0.53 |
0.44 |
0.82 |
|
| Intention |
Before |
55.73 (4.1) |
53.28 (4.61) |
55.78 (2.66) |
55.63 (2.87) |
0.73 |
| Behavior |
After |
2.54 (1.17) |
2.80 (0.98) |
2.87 (0.99) |
2.31 (0.94) |
0.35 |
Note. SD: Standard deviation; ANOVA: Analysis of variance; EPPM: Extended parallel process model. *Intervention 1: Gain-frame messages; Intervention 2: Loss-frame messages; Intervention 3: Both messages **One-way ANOVA; ***Paired sample t-test.
Discussion
Despite the negative effects of inappropriate CF, many mothers abandon exclusive breastfeeding prematurely and feed their infants inappropriate foods, justifying the need for health education interventions. On the other hand, various studies have shown different and sometimes contradictory effects of gain and loss messages commonly used in health education. Therefore, this study evaluated the effect of different types of messages (gain frame, loss frame, and a combination of both) on the knowledge, attitudes, and behavior of mothers in Jahrom.
The results of the current study indicated that the educational intervention, regardless of whether it used the gain frame, the loss frame, or a combination of both, significantly increased mean knowledge scores in all three intervention groups. However, no significant increase in knowledge was observed in the control group. This result is consistent with the findings of Rafiyan et al (33), demonstrating an increase in knowledge following educational interventions in different experimental groups. Despite the significant improvements in knowledge in each of the intervention groups, there were no significant differences between the gain, loss, and combined message groups. This suggests that in the context of CF education, the type of informational framework may not significantly influence the degree of knowledge gain.
In terms of perceived susceptibility, within-group comparisons showed a significant increase in the mean value of perceived susceptibility in all intervention groups. However, no significant differences were found between the experimental groups and the control group, which contradicts the results of Alidosti et al (35), indicating a significant increase in perceived susceptibility in their intervention groups after the intervention. As perceived susceptibility tends to be contextual and subjective, it may be influenced by other factors, such as the timing of the intervention or mothers’ specific concerns about CF, which were not examined in this study.
The results for perceived severity were somewhat inconclusive. In the present study, no significant changes in perceived severity were detected in any of the groups, which does not match the results of studies by Zareharofteh and Karimi (32) and Alidosti et al (35), reporting a significant increase in perceived severity in the intervention groups. The contradictions between these studies and the current study may be due to differences in the target population, the cultural context, or the specific communication strategies used. It is possible that the severity of the risks associated with inappropriate CF was not perceived as urgently as in other contexts or that the messages used were not strong enough to significantly change the perceived severity.
With regard to self-efficacy, the results revealed that the mean self-efficacy scores increased significantly in all three intervention groups, while no significant changes were observed in the control group. However, there were no significant differences in the increase in self-efficacy scores between different groups with a variety of message frames, which is in line with the findings of Rafiyan et al (33) and Alidosti et al (35), demonstrating no significant differences in self-efficacy between participants exposed to the gain or loss messages. On the other hand, Zareharofteh and Karimi (32) reported that self-efficacy was significantly higher in the group exposed to gain messages than in the group exposed to loss messages. This discrepancy could be due to the nature of the intervention, the specific target behavior, or the inherent differences in participants’ responses to positive and negative framing in different contexts.
No significant changes were found in the mean values of response efficacy within or between the groups, which is in contrast to the results of Zareharofteh and Karimi (32) and Alidosti et al (35), confirming an increase in response efficacy both in a gain frame and after the use of the loss frame. One possible explanation for this difference could be the nature of the content of the message, which may not have been persuasive enough or tailored enough to enhance the response efficacy of recommended behaviors. Alternatively, other variables, such as personal beliefs or external support systems, may have played a more important role in shaping response efficacy in the current study.
Finally, our results showed no significant differences in mothers’ behavior regarding CF practices after the intervention, regardless of whether they received a gain frame, a loss frame, or a combined message, which contradicts the results of the study by Rafiyan et al (33), indicating that the messages with the loss frame had a significant effect on mothers’ CF behavior. The lack of significant behavior change in the current study could be due to the short duration of the intervention, the need for additional reinforcement, or the complexity of behavior change in the context of CF. It is possible that while knowledge and attitudes were influenced, more intensive or longer-term interventions would be required for substantial behavior change.
Strengths and Limitations
This study has several strengths, including the use of a factorial design that allows for a comprehensive examination of the effects of different messages (gain, loss, and combination) on mothers’ knowledge, attitudes, and behaviors related to complementary foods. However, there are also notable limitations. The intervention was delivered to mothers with infants aged 2–4 months, which may have been too late to observe significant behavioral changes, suggesting that earlier interventions, such as immediately after birth or during pregnancy, may be more effective. In addition, the study had a short follow-up period, limiting the ability to assess the long-term effects of the intervention. While the factorial design provides valuable insights, refining the content of the message to ensure that greater differentiation and impact could improve the results of future studies.
Conclusion
Several studies have shown that message framing can influence knowledge, attitudes, and behaviors related to health practices. However, the results of this study revealed that the type of message (gain frame, loss frame, or both) did not lead to significant differences in key behavioral outcomes related to CF. The findings highlight the need for further research to better understand factors that contribute to effective health education, including the potential role of contextual and individual differences in message uptake. Future interventions could benefit from a tailored approach that considers both the content and delivery of messages to more effectively promote positive maternal health behaviors.
Theoretical Implications
This study suggests that the effects of message framing on health behavior may depend on contextual and individual factors, not just the type of applied frame. It underlines the need for a more comprehensive theoretical framework that incorporates timing, content, and audience characteristics to understand the effectiveness of health communication.
Practical Implications
In practice, the study recommends that health education interventions about CF should be more tailored to individual needs and cultural contexts. Future interventions should consider the timing, duration, and methods of communication to increase their effectiveness and promote long-term behavior change.
Acknowledgements
This study was approved and supported by Shiraz University of Medical Sciences, Shiraz, Iran. It was not possible without the support of Jahrom University of Medical Sciences. The authors would like to thank all the personnel of comprehensive health centers who cooperated with us in this study and the mothers who participated in this project.
Competing Interests
The authors declare that they have no competing interests in this section.
Ethical Approval
This study is based on the research plan approved by the Ethics Committee of Shiraz University of Medical Sciences (ethical code IR. SUMS.SCHEANUT.1401.029). Ethical standards, such as obtaining informed consent, ensuring privacy, and maintaining confidentiality, were followed in this study. Informed consent was obtained from all study participants.
Funding
This study was self-funded by the authors and received no external financial support from any funding organization.
References
- Schwarzenberg SJ, Georgieff MK. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 2018; 141(2):e20173716. doi: 10.1542/peds.2017-3716 [Crossref] [ Google Scholar]
- FAO, IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2020: Transforming Food Systems for Affordable Healthy Diets. Rome, FAO; 2020. doi: 10.4060/ca9692en.
- Czosnykowska-Łukacka M, Królak-Olejnik B, Orczyk-Pawiłowicz M. Breast milk macronutrient components in prolonged lactation. Nutrients 2018; 10(12):1893. doi: 10.3390/nu10121893 [Crossref] [ Google Scholar]
- Infant Food and Feeding. American Academy of Pediatrics. Available from: https://scholar.google.com/scholar?cites=11613768690944367795&as_sdt=2005&sciodt=0,5&hl=en. Updated 07/06/2021.
- de Oliveira MM, Daher DV, da Silva JL, de Araújo Andrade SS. Men’s health in question: seeking assistance in primary health care. Cien Saude Colet 2015; 20(1):273-8. doi: 10.1590/1413-81232014201.21732013 [Crossref] [ Google Scholar]
- Dewey K. Guiding Principles for Complementary Feeding of the Breastfed Child. WHO; 2003.
- Kostecka M, Jackowska I, Kostecka J. Factors affecting complementary feeding of infants a pilot study conducted after the introduction of new infant feeding guidelines in Poland. Nutrients 2020; 13(1):61. doi: 10.3390/nu13010061 [Crossref] [ Google Scholar]
- Binns C, Lee MK, Yun Low W, Baker P, Bulgiba A, Dahlui M. Guidelines for complementary feeding of infants in the Asia Pacific region: APACPH Public Health Nutrition Group. Asia Pac J Public Health 2020; 32(4):179-87. doi: 10.1177/1010539520931328 [Crossref] [ Google Scholar]
- Dewey KG, Adu-Afarwuah S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr 2008; 4(Suppl 1):24-85. doi: 10.1111/j.1740-8709.2007.00124.x [Crossref] [ Google Scholar]
- Matvienko-Sikar K, Kelly C, Sinnott C, McSharry J, Houghton C, Heary C. Parental experiences and perceptions of infant complementary feeding: a qualitative evidence synthesis. Obes Rev 2018; 19(4):501-17. doi: 10.1111/obr.12653 [Crossref] [ Google Scholar]
- Uvere PO, Ene-Obong HN. Complementary local foods for infants in developing countries. In: Watson RR, Grimble G, Preedy VR, Zibadi S, eds. Nutrition in Infancy: Volume 1. Totowa, NJ: Humana Press; 2013. p. 75-93. doi: 10.1007/978-1-62703-224-7_6.
- Arden MA. Conflicting influences on UK mothers’ decisions to introduce solid foods to their infants. Matern Child Nutr 2010; 6(2):159-73. doi: 10.1111/j.1740-8709.2009.00194.x [Crossref] [ Google Scholar]
- Hamilton K, Daniels L, Murray N, White KM, Walsh A. Mothers’ perceptions of introducing solids to their infant at six months of age: identifying critical belief-based targets to promote adherence to current infant feeding guidelines. J Health Psychol 2012; 17(1):121-31. doi: 10.1177/1359105311409786 [Crossref] [ Google Scholar]
- Kazemi SM, Ghahremani L, Karimi M, Fararouei M, Zare E. Effect of the planned behavior-based education intervention on timely initiation of infants’ complementary feeding in primiparous mothers; a randomized controlled trial. Health Educ Health Promot 2022; 10(1):75-81. [ Google Scholar]
- Salarkia N, Amini M, Eslami Amirabadi M, Dadkhah M, Zowghi T, Heidari H, et al. Mothers’ views and beliefs about the role of complementary feeding in children under the age of two in Damavand: a qualitative study. J Arak Uni Med Sci 2010;13(2):63-74. [Persian].
- Prescott SL, Smith P, Tang M, Palmer DJ, Sinn J, Huntley SJ. The importance of early complementary feeding in the development of oral tolerance: concerns and controversies. Pediatr Allergy Immunol 2008; 19(5):375-80. doi: 10.1111/j.1399-3038.2008.00718.x [Crossref] [ Google Scholar]
- Chehab RF, Cross TL, Forman MR. The gut microbiota: a promising target in the relation between complementary feeding and child undernutrition. Adv Nutr 2021; 12(3):969-79. doi: 10.1093/advances/nmaa146 [Crossref] [ Google Scholar]
- Danaei G, Andrews KG, Sudfeld CR, Fink G, McCoy DC, Peet E. Risk factors for childhood stunting in 137 developing countries: a comparative risk assessment analysis at global, regional, and country levels. PLoS Med 2016; 13(11):e1002164. doi: 10.1371/journal.pmed.1002164 [Crossref] [ Google Scholar]
- Królak-Olejnik B, Błasiak I, Szczygieł A. Promotion of breastfeeding in Poland: the current situation. J Int Med Res 2017; 45(6):1976-84. doi: 10.1177/0300060517720318 [Crossref] [ Google Scholar]
- Blaney S, Februhartanty J, Sukotjo S. Feeding practices among Indonesian children above six months of age: a literature review on their magnitude and quality (part 1). Asia Pac J Clin Nutr 2015; 24(1):16-27. doi: 10.6133/apjcn.2015.24.1.13 [Crossref] [ Google Scholar]
- Behzadifar M, Saki M, Behzadifar M, Mardani M, Yari F, Ebrahimzadeh F. Prevalence of exclusive breastfeeding practice in the first six months of life and its determinants in Iran: a systematic review and meta-analysis. BMC Pediatr 2019; 19(1):384. doi: 10.1186/s12887-019-1776-0 [Crossref] [ Google Scholar]
- Zarshenas M, Zhao Y, Scott JA, Binns CW. Determinants of breastfeeding duration in Shiraz, Southwest Iran. Int J Environ Res Public Health 2020; 17(4):1192. doi: 10.3390/ijerph17041192 [Crossref] [ Google Scholar]
- Ghahremani L, Hemmati N, Kaveh MH, Fararoei M. Effects of an educational intervention targeting body image on self-esteem of Iranian high-school students: a quasi-experimental trial. Arch Psychiatry Psychother 2018; 1:59-66. doi: 10.12740/app/81549 [Crossref] [ Google Scholar]
- Ruiter RA, Kessels LT, Peters GJ, Kok G. Sixty years of fear appeal research: current state of the evidence. Int J Psychol 2014; 49(2):63-70. doi: 10.1002/ijop.12042 [Crossref] [ Google Scholar]
- Witte K. Putting the fear back into fear appeals: the extended parallel process model. Commun Monogr 1992; 59(4):329-49. doi: 10.1080/03637759209376276 [Crossref] [ Google Scholar]
- Witte K. Fear control and danger control: a test of the extended parallel process model (EPPM). Commun Monogr 1994; 61(2):113-34. doi: 10.1080/03637759409376328 [Crossref] [ Google Scholar]
- Barnett DJ, Balicer RD, Thompson CB, Storey JD, Omer SB, Semon NL. Assessment of local public health workers’ willingness to respond to pandemic influenza through application of the extended parallel process model. PLoS One 2009; 4(7):e6365. doi: 10.1371/journal.pone.0006365 [Crossref] [ Google Scholar]
- Popova L. The extended parallel process model: illuminating the gaps in research. Health Educ Behav 2012; 39(4):455-73. doi: 10.1177/1090198111418108 [Crossref] [ Google Scholar]
- Carcioppolo N, Jensen JD, Wilson SR, Collins WB, Carrion M, Linnemeier G. Examining HPV threat-to-efficacy ratios in the Extended Parallel Process Model. Health Commun 2013; 28(1):20-8. doi: 10.1080/10410236.2012.719478 [Crossref] [ Google Scholar]
- Mohammadi A, Karimi M, Hashemi H, Asadollahi A. An educational intervention based on extended parallel model to reduce exposure of pregnant women to BTEX air pollutants: a quasi-experimental study. Health Care Women Int. 2024:1-16. doi: 10.1080/07399332.2024.2433997.
- Pavey L, Churchill S. Promoting the avoidance of high-calorie snacks: priming autonomy moderates message framing effects. PLoS One 2014; 9(7):e103892. doi: 10.1371/journal.pone.0103892 [Crossref] [ Google Scholar]
- Zareharofteh F, Karimi M. Impacts of gain versus loss frame messages about beverages on boy students, an application of extended parallel process model. J Health Popul Nutr 2022; 41(1):23. doi: 10.1186/s41043-022-00301-1 [Crossref] [ Google Scholar]
- Rafieyan-Kopaei Z, Fathian-Dastgerdi Z, Tarrahi MJ, Zamani-Alavijeh F. Effectiveness of message-framing intervention on complementary feeding related behaviors among mothers with infants aged 4-8 months: a 3-arm randomized controlled trial. Ital J Pediatr 2019; 45(1):158. doi: 10.1186/s13052-019-0749-0 [Crossref] [ Google Scholar]
- Ghodsi D, Omidvar N, Rashidian A, Eini-Zinab H, Raghfar H, Aghayan M. Effectiveness of the national food supplementary program on children growth and nutritional status in Iran. Matern Child Nutr 2018; 14(3):e12591. doi: 10.1111/mcn.12591 [Crossref] [ Google Scholar]
- Alidosti M, Shahnazi H, Heidari Z, Zamani-Alavijeh F. Design and evaluation of two educational media in the form of animation and games to promote the cutaneous leishmaniasis prevention behaviors in adolescent female. BMC Public Health 2022; 22(1):2288. doi: 10.1186/s12889-022-14772-8 [Crossref] [ Google Scholar]