J Educ Community Health. 12(2):122-131.
doi: 10.34172/jech.3356
Review Article
Effects of Different Sedentary Interruption Interventions on Vascular Function in Adults: A Network Meta-Analysis
Tongyan Zhang Conceptualization, Formal analysis, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing, 1 
Anastasiia V. Kabachkova Conceptualization, Resources, Supervision, Writing – review & editing, 1, 2, *
Xianbo Qu Formal analysis, Investigation, Methodology, 1
Author information:
1Faculty of Physical Education, Tomsk State University, Tomsk 634050, Russia
2Institute of Integrative Healthcare, Siberian State Medical University, Tomsk 634050, Russia
Abstract
Background: Interrupting sedentary behavior through intermittent activity may prevent or ameliorate vascular dysfunction. This study aimed to compare and rank the effectiveness of different sedentary interruption interventions on vascular function in adults using a network meta-analysis (NMA).
Methods: A systematic search was conducted in PubMed, Cochrane, Embase, and Web of Science databases to identify the randomized controlled trials that investigated the impact of sedentary interruption interventions on adult vascular function. The retrieval period was from inception to October 2024. Paired analyses and NMAs were conducted using the random-effects model.
Results: This research included 27 studies, which involved five sedentary intervention methods and covered a total of 483 participants. Sedentary interruption interventions can effectively improve the levels of blood flow (mean difference [MD] = 0.33, 95% confidence interval [CI]: 0.18, 0.48), mean arterial shear rate (MD = 0.32, 95% CI: 0.15 0.49), flow-mediated dilation (FMD)% (MD = 0.43, 95% CI: 0.26, 0.59), and carotid-to-ankle pulse-wave velocity (PWV; MD = -1.12, 95% CI: -1.50, -0.73). The surface under the cumulative ranking curve revealed that aerobic activities were the most effective interventions in improving mean arterial pressure, blood flow, and mean arterial shear rate. Lower-extremity activities could most effectively improve FMD%, carotid-to-ankle PWV, and carotid-to-femoral PWV, and standing achieved good results in improving carotid-to-radial PWV.
Conclusion: Interventions to interrupt sedentary behavior effectively enhance vascular health in sedentary populations. Aerobic activities and lower-extremity activities have demonstrated relatively strong advantages in improving vascular function.
Keywords: Sedentary behavior, Vascular function, Pulse-wave velocity, Flow-mediated dilation, Shear rate
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Zhang T, Kabachkova AV, Qu X. Effects of different sedentary interruption interventions on vascular function in adults: a network meta-analysis. J Educ Community Health. 2025; 12(2):122-131. doi:10.34172/jech.3356
Introduction
Sedentary behavior is defined as any awake activity with an energy expenditure of less than 1.5 metabolic equivalents (1). Advances in modern society have reduced the demand for physical labor, resulting in individuals spending most of their waking hours sedentary, thus making it the most prevalent form of inactivity (2). It is reported that the average sedentary time for adults exceeds 8 hours (3,4). An increasing body of evidence suggests that prolonged sedentary behavior heightens the risk of various cardiovascular diseases (CVDs), including coronary artery disease, myocardial infarction, and ischemic stroke (5,6). Specifically, prolonged sitting (ranging from 3 hours to 5 hours) has been associated with increases in diastolic blood pressure and mean arterial pressure (7). This comportment can adversely affect lower limb flow-mediated dilation (FMD) (8) and carotid-femoral pulse-wave velocity (PWV). From a physiological perspective, this may be due to the lack of leg muscle activity during sitting, leading to venous pooling in the lower limbs. This pooling reduces venous return, subsequently decreasing cardiac output. A reduction in cardiac output results in decreased shear stress from lower limb blood flow, which further lowers the bioavailability of nitric oxide, impairing endothelial function and ultimately contributing to arterial stiffness (9,10). The detrimental effects of sedentary behavior on hemodynamics and vascular function are considered potential contributors to the increased incidence and mortality risk associated with CVDs. Consequently, reducing sedentary behavior and conducting active interventions are of crucial importance for improving or maintaining the cardiovascular function of sedentary individuals and for preventing and treating CVDs, such as atherosclerosis.
As sedentary behavior trends increase globally, the World Health Organization has published guidelines on physical activity and sedentary behavior (11). Interventions that break sedentary time and increase physical activity have gained recognition for improving and maintaining vascular function, as well as preventing and treating CVDs (1,12). Numerous studies have confirmed that breaking sedentary behavior positively influences vascular function. For example, intermittent stair climbing has been shown to enhance arterial blood flow and shear rate (13). Furthermore, taking standing breaks from prolonged sitting has been associated with reductions in diastolic blood pressure, mean arterial pressure, and ankle-brachial index (7), thereby facilitating improved vasodilation (14). However, some research presents contrasting findings, indicating no significant difference in FMD between interrupted and uninterrupted sedentary behavior (15,16). This discrepancy suggests that variability in results may be influenced by different interruption strategies employed across studies.
Although the majority of randomized controlled trials (RCTs) and meta-analyses have hitherto demonstrated the impact of sedentary interruption on cardiovascular health (16,17), the inconsistency in research findings indicates that numerous uncertainties remain in aspects such as the specific action mechanisms of different intervention measures on cardiovascular function and the stability of their effects. Moreover, pairwise meta-analysis is unable to rank the efficacy of different intervention measures, nor can it determine which interruption approach is more effective in improving vascular function outcomes. Consequently, network meta-analysis (NMA) was adopted in this study. It aims to integrate various sedentary interruption strategies and conduct a comprehensive comparison of the advantages and effectiveness of results related to vascular function, with the intention of providing valuable insights into the optimal sedentary intervention strategies for improving vascular function and reducing the risk of CVDs.
Materials and Methods
Registration
This systematic review and NMA will be reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (18,19). The relevant protocol has been registered with the International Prospective Register of Systematic Reviews (CRD42024612095).
Search Strategy
Systematic searches were conducted in Embase, PubMed, Cochrane Library, and Web of Science databases for studies investigating the effect of sedentary interruption on vascular function in adults up to October 2024. Search terms were classified under the Population, Intervention, Comparison, Outcomes, and Study framework using a combination of keywords and free terms. The main search terms (Table S1) were adults (P), intermittent (I), sedentary (C), and vascular function parameters, including blood flow, PWV, and FMD, shear rate, among others (O).
Study Selection and Eligibility Criteria
The searched studies were imported into EndNote 21, and duplicates were removed. Two researchers (Z and Q) independently screened the literature based on the inclusion and exclusion criteria. The inclusion criteria were study type (RCTs, randomized crossover trials, and human studies) and study population (adults aged 18 and above). There were no predetermined restrictions regarding health or disease status, thereby avoiding the unnecessary exclusion of any potentially valuable data. The other inclusion criteria included intervention type (any sedentary interruption intervention involving multiple bouts of movement, including standing, with a control group remaining in continuous sedentary behavior) and outcome measures (they had to include at least one vascular function outcome, specifically mean arterial pressure, blood flow, mean arterial shear rate, PWV, and FMD). On the other hand, the exclusion criteria were (1) systematic reviews, meta-analyses, conference abstracts, and study protocols, (2) animal studies, (3) duplicates, and (4) inaccessible full texts or relevant information. Literature search and screening were independently conducted by two researchers (Z and Q), and any discrepancies were resolved through discussion or consultation with a third reviewer to reach a consensus.
Data Extraction
The data from eligible studies were independently extracted and organized into Excel 2019 by two reviewers (Z and Q), including basic information, participant information, exercise intervention details, and outcome measures. Basic information included title, first author, publication year, and study type, and participant information contained country, average age, sample size, and health profile. The health profile encompasses both the health state (the absence of diagnosed diseases) and the disease state (e.g., obesity, overweight, diabetes mellitus, and the like). Exercise intervention details encompassed the type of sedentary interruption, total sedentary duration, interruption frequency, number of interruptions, duration, and intensity. Finally, outcome measures were mean arterial pressure, blood flow, mean arterial shear rate, PWV, and FMD. As mentioned earlier, the required data were extracted by two researchers, and any discrepancies were resolved through discussion or consultation with a third reviewer to reach a consensus.
Risk of Bias and Quality Assessment
The risk of bias in the included RCTs was assessed employing the revised Cochrane risk-of-bias (RoB) tool for randomized trials (20). The included studies were assessed for quality from the different aspects, including (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result. For each domain, predefined signaling questions were answered with “Yes”, “Probably Yes”, “No”, “Probably No”, and “No Information” options. The risk-of-bias judgments for each domain were “low risk of bias”, “some concerns”, or “high risk of bias.” Quality assessment was conducted independently by two researchers (Z and Q). Should any discrepancies arise, a consensus was reached through discussion or consultation with a third reviewer.
Data Synthesis and Analysis
The corresponding processing methods were adopted according to the data type. Means and standard deviations (SD) were extracted for continuous data. For data with medians and interquartile ranges, means were estimated by (first quartile + third quartile) ÷ 2, and SDs were estimated by (third quartile - first quartile) ÷ 1.35 (21). For data presenting 95% confidence intervals (CIs), the standard errors (SE) were estimated by (upper limit - lower limit) ÷ 3.92, and SDs were as SE × √n (22).
Based on the different sedentary interruption intervention measures included in the studies, a network graph was constructed to display the relationships among these intervention measures. The network graph illustrated the connections between various training interventions, with nodes representing different interventions and edges depicting the connections or relationships between them. Pairwise meta-analyses were conducted for each intervention comparison. The MD and 95% CI were utilized to analyze continuous data for representing the effect size, and the I2 statistic was employed to assess the heterogeneity of treatment effects. When the I2 exceeded 50%, the heterogeneity was regarded as significant. An NMA was performed using a random-effects model based on the Bayesian framework. This model adopted the Markov Chain Monte Carlo method to obtain non-informative uniform and normal prior distributions. For model parameters, four chains were used (23,24), with a step size of 1, an annealing count of 20,000, and a simulation iteration of 50,000 (25). The deviance information criterion (DIC) was utilized to assess model fit. A DIC value of less than 10 was considered to indicate no significant global inconsistency. When the network diagram had a closed loop, local inconsistency was examined through node-splitting analysis; if the P-value was less than 0.05, it indicated significant local inconsistency (26). Surface under the cumulative ranking curve (SUCRA) is a quantitative indicator for comparing the superiority and inferiority of the effects of multiple intervention measures. The rankings among various sedentary interruption measures were obtained by the area under the SUCRA in the cumulative probability plot. The value of SUCRA ranges from 0% to 100%, and a larger value indicates that the intervention measure is more effective (27). For publication bias, visual inspection was conducted using funnel plots and evaluation through Egger’s test (28). Publication bias was considered absent when the symmetry of the funnel plot was inspected visually or when the P-value was greater than 0.05. The network map command in Stata 16.0 (version 16.1; Stata Corporation, College Station, TX, USA) was employed to generate network diagrams, funnel plots, and cumulative probability plots. League tables and probability ranking tables were created using the gemtc package and rjags package in RStudio (version 1.2.5042, 2020; RStudio, Inc., Boston, MA, USA) software.
Results
Study Selection
A total of 3570 articles were retrieved from the database. After importing into EndNote 21 and removing 1405 duplicates and 278 articles flagged as ineligible by automated tools, an initial screening through title and abstract review excluded 1833 articles that were reviews, animal studies, non-RCTs, or non-randomized crossover trials. Overall, 54 articles remained for further examination. After reading the full text, 20 articles were excluded due to missing data, non-independent exercise interventions, or a lack of vascular function outcome measures. Finally, 27 articles were included in the systematic review and NMA. The PRISMA flow diagram is presented in Figure 1.
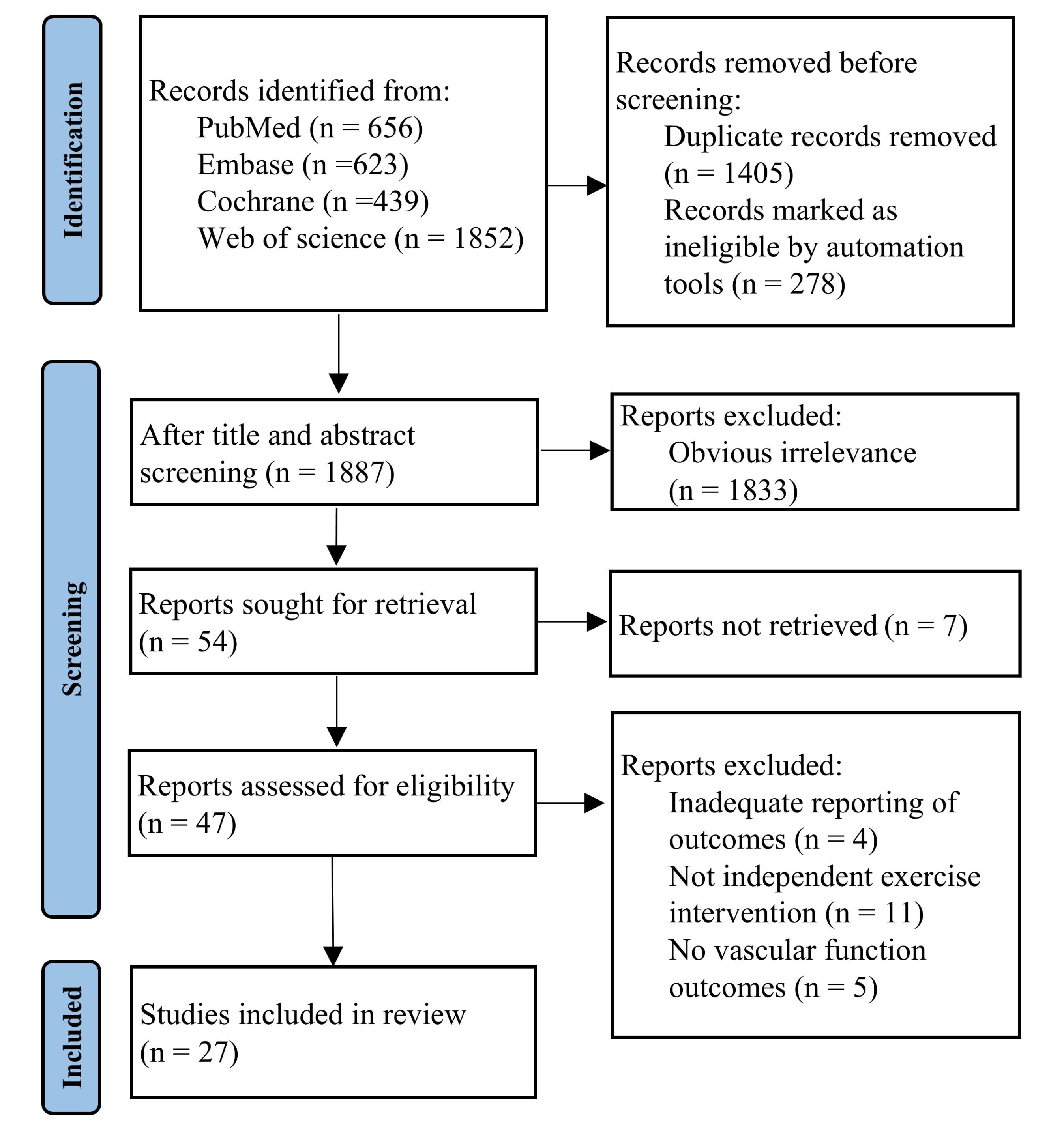
Figure 1.
PRISMA Flow Diagram of the Study Selection Process. Note. PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
.
PRISMA Flow Diagram of the Study Selection Process. Note. PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
Characteristics of the Included Studies
This study included 27 research articles with a total of 483 participants, averaging 35.06 ± 6.79 years in age and comprising 263 males and 220 females. The distribution of study subjects by country included Brazil, Canada, Italy, New Zealand, the Netherlands, and South Korea (1 study each), Japan and the United Kingdom (3 studies each), Australia (5 studies), and the America (10 studies). The experimental group engaged in five types of sedentary interruption interventions, including aerobic activities (7 studies), resistance activities (5 studies), lower-extremity activities (7 studies), standing (4 studies), and walking (8 studies), while the control group continued sedentary behavior. The basic characteristics of the included studies are presented in Table S2.
Risk of Bias Quality Evaluation
Among the 27 studies included in this research, 37%, 59.3%, and 3.7% were assessed as having “low risk”, “some risk”, and “high risk” of bias, respectively. For the randomization process, 37%, 59.3%, and 3.7% had “low risk”, “some risk”, and “high risk” of bias, respectively. Regarding deviations from intended interventions, 96.3% were “low risk”, with 3.7% at “some risk”. All studies presented “low risk” for outcome data missingness (100%), outcome measurement (100%), and selective reporting (100%). The primary risk sources included 10 studies that reported random allocation methods via random number generation, coin tossing, or computer programs, while 2 studies utilized independent personnel for random grouping. Further, 15 studies did not provide detailed descriptions of randomization methods. Blinding of exercise intervention allocation posed challenges in exercise-related studies, resulting in only 4 studies reporting blinding (3 double-blind, 1 single-blind), with others lacking detailed descriptions. All studies achieved a participant retention rate of 95% (or 90%), with few cases of missing outcome data. Appropriate outcome measurement methods were employed, mitigating the risk of selective reporting. Figure S1 displays the RoB diagram.
Pairwise Meta-Analysis and Network Meta-Analysis
The 27 included studies discussed five different sedentary interruption interventions, including aerobic activities, lower-extremity activities, resistance activities, standing, and walking. The network structure diagram illustrating the relationships between these interventions is presented in Figure 2A-G. The thickness of the lines in the diagram reflects the number of pairwise comparisons among the interventions. Additionally, the size of the circles representing the interventions can be proportional to the number of participants included in each intervention. The difference in DIC values between the consistency model and the inconsistency model was less than 5, and the I2 values of all outcomes were less than 25%, indicating the absence of global inconsistency. The global inconsistency and heterogeneity of each outcome are provided in Table S3. There were some closed-loop network structures in the comparison of blood flow, mean arterial shear rate, and FMD. Local inconsistency was found in blood flow (standing vs. aerobic activities, P = 0.007) and mean arterial shear rate (walking vs. aerobic activities, P = 0.005) by the node-splitting method. The node-splitting results of all outcomes are summarized in Table S4.
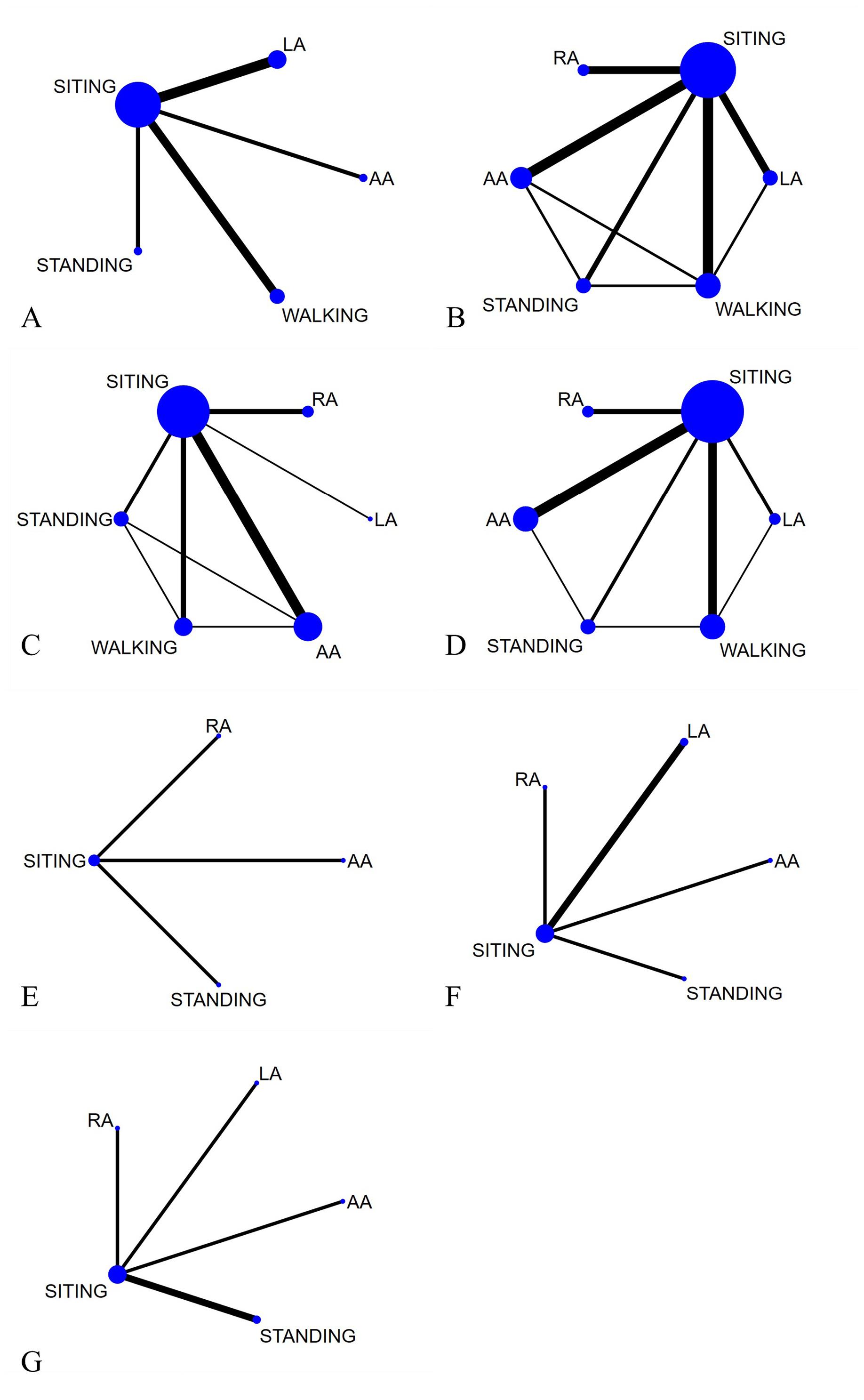
Figure 2.
Network Graph: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, (D) Flow-Mediated Dilation%, (E) Carotid-to-Radial PWV, (F) Carotid-to-Ankle PWV, and (G) Carotid-to-Femoral PWV. Note. Each node represents one activity type. The lines between the dots indicate a direct comparison between the two modes of motion, with thicker lines for more studies and thinner lines for fewer studies. PWV: Pulse-wave velocity; AA: Aerobic activities; RA: Resistance activities; LA: Lower-extremity activities
.
Network Graph: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, (D) Flow-Mediated Dilation%, (E) Carotid-to-Radial PWV, (F) Carotid-to-Ankle PWV, and (G) Carotid-to-Femoral PWV. Note. Each node represents one activity type. The lines between the dots indicate a direct comparison between the two modes of motion, with thicker lines for more studies and thinner lines for fewer studies. PWV: Pulse-wave velocity; AA: Aerobic activities; RA: Resistance activities; LA: Lower-extremity activities
Mean Arterial Pressure
Mean arterial pressure was reported in 13 studies involving 516 participants and four sedentary interruption interventions (i.e., aerobic activities, lower-extremity activities, standing, and walking). The results of the pairwise meta-analysis showed that the sedentary interruption interventions were not statistically significant compared to the control group (MD = 0.15; 95% CI: -0.03, 0.33; P = 0.00; I2 = 62.8%, Figure S2). Based on NMA based concordance analysis, compared to prolonged sitting, intermittent aerobic activities (MD = 2.03, 95% CI: 0.22, 4.19) demonstrated a greater advantage in improving mean arterial pressure in adults. Lower extremity activities (MD = 0.61, 95% CI: -1.48, 2.67), standing (MD = -0.27, 95% CI: -2.54, 1.62), and walking (MD = -0.06, 95% CI: -1.37, 1.58) indicated no statistically significant difference in results compared to the control group. Similarly, indirect comparisons between the two revealed no statistically significant differences between the two sedentary interruption intercomparisons (Table S5). The ranking order of effectiveness for improving mean arterial pressure across different interventions was aerobic activities (SUCRA = 0.947), lower-extremity activities (SUCRA = 0.585), and walking (SUCRA = 0.331) (Figure 3A).
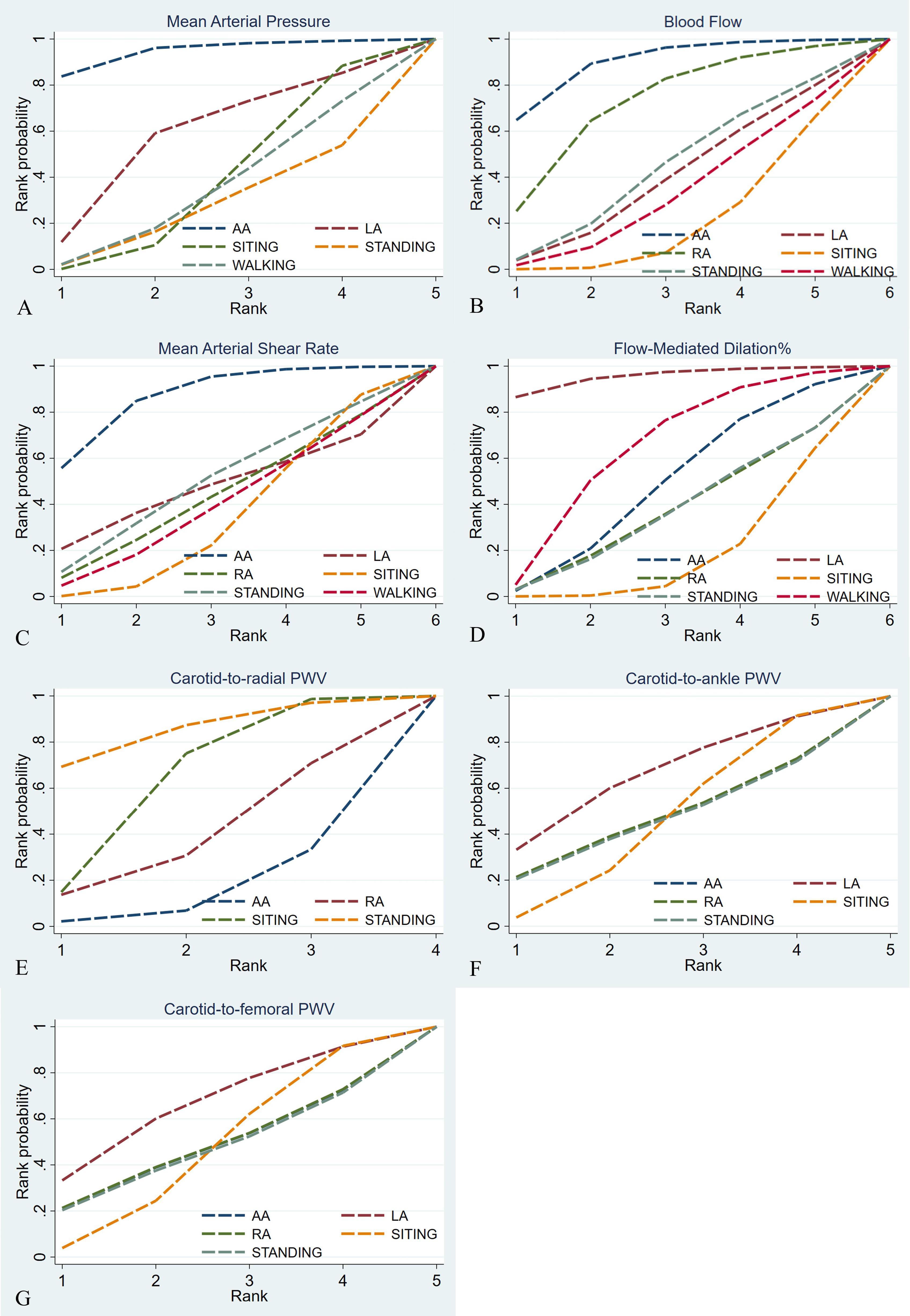
Figure 3.
Cumulative Ranking Probability Graph: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, (D) Flow-Mediated Dilation%, (E) Carotid-to-Radial PWV, (F) Carotid-to-Ankle PWV, and (G) Carotid-to-Femoral PWV. Note. The surface under the cumulative ranking curve value is the probability each treatment has of being among the best of those in the network, with larger values representing higher ranking probabilities. PWV: Pulse-wave velocity; AA: Aerobic activities; RA: Resistance activities; LA: Lower-extremity activities
.
Cumulative Ranking Probability Graph: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, (D) Flow-Mediated Dilation%, (E) Carotid-to-Radial PWV, (F) Carotid-to-Ankle PWV, and (G) Carotid-to-Femoral PWV. Note. The surface under the cumulative ranking curve value is the probability each treatment has of being among the best of those in the network, with larger values representing higher ranking probabilities. PWV: Pulse-wave velocity; AA: Aerobic activities; RA: Resistance activities; LA: Lower-extremity activities
Blood Flow
Blood flow was reported in 12 studies involving 538 participants and five sedentary interruption interventions (i.e., aerobic activities, resistance activities, lower-extremity activities, standing, and walking). The results of the pairwise meta-analysis demonstrated that sedentary interruption interventions effectively improved blood flow in the intervention group (MD = 0.33; 95% CI: 0.18, 0.48; P = 0.0; I2 = 73.5%, Figure S3). NMA-based concordance analysis showed that, compared to prolonged sitting, intermittent aerobic activity (MD = 48.6, 95% CI: 7.53, 90.59) confirmed a significant advantage in improving blood flow in adults. Resistance activities (MD = 32.91, 95% CI: -10.89, 77.12), lower-extremity activities (MD = 9.73, 95% CI: -32.53, 38.26), standing (MD = 13.01, 95% CI: -35.34, 59.23), and walking (MD = 5.59, 95% CI: -38.32, 44.8) revealed no statistically significant difference in results compared to the control group. Indirect comparisons between the two represented no statistically significant differences between the two sedentary interruption intercomparisons (Table S6). The ranking order of effectiveness for improving blood flow was aerobic activities (SUCRA = 0.898), resistance activities (SUCRA = 0.723), and standing (SUCRA = 0.443), respectively (Figure 3B).
Mean Arterial Shear Rate
Mean arterial shear rate was reported in 12 studies involving 454 participants and five sedentary interruption interventions (i.e., aerobic activities, resistance activities, lower-extremity activities, standing, and walking). Based on the results of the pairwise meta-analysis, sedentary interruption interventions could effectively improve mean arterial shear rate in the intervention group (MD = 0.32; 95% CI: 0.15, 0.49; P = 0.0; I2 = 88.2%, Figure S4). NMA-based concordance analysis indicated that intermittent aerobic activity (MD = 75.94, 95% CI: 3.68, 153.61), compared to prolonged sitting, demonstrated a significant advantage in improving mean arterial shear rate in adults. Lower-extremity activities (MD = 13.7, 95% CI: -170.78, 198.29), resistance activities (MD = 9.13, 95% CI: -98.77, 117.57), standing (MD = 18.92, 95% CI: -99.1, 138.67), and walking (MD = 4.07, 95% CI: -98.59, 107.37) showed no statistically significant difference in results in comparison to the control group. Based on indirect comparisons, no statistically significant differences were observed between the two sedentary interruption intercomparisons (Table S7). The effectiveness ranking for improving mean arterial shear rate was aerobic activities (SUCRA = 0.868), standing (SUCRA = 0.496), and lower-extremity activities (SUCRA = 0.468), respectively (Figure 3C).
Flow-Mediated Dilation (%)
FMD% was observed in 15 studies involving 531 participants and five sedentary interruption interventions (i.e., aerobic activities, resistance activities, lower-extremity activities, standing, and walking). According to the results of the pairwise meta-analysis, sedentary interruption interventions led to an effective improvement in FMD% in the intervention group (MD = 0.43; 95% CI: 0.26, 0.59; P = 0.0; I2 = 88.6%, Figure S5). NMA-based concordance analysis revealed intermittent lower-extremity activities (MD = 3.86, 95% CI: 0.77, 6.84) improved FMD% compared to prolonged sitting. Aerobic activities (MD = 0.9, 95% CI: -0.97, 2.75), resistance activities (MD = 0.49, 95% CI: -2.1, 3.11), standing (MD = 0.5, 95% CI: -2.26, 3.24), and walking (MD = 1.51, 95% CI: -0.5, 3.42) showed no statistically significant difference in results compared to the control group. Based on indirect comparisons, there were no statistically significant differences between the two sedentary interruption intercomparisons (Table S8). The ranking order of effectiveness for improving FMD% was lower-extremity activities (SUCRA = 0.953), walking (SUCRA = 0.639), and aerobic activities (SUCRA = 0.482), respectively (Figure 3D).
Pulse-Wave Velocity
Carotid-to-radial PWV was found in 3 studies involving 120 participants and three sedentary interruption interventions (i.e., aerobic activities, resistance activities, and standing). The results of the pairwise meta-analysis indicated that the sedentary interruption interventions were not statistically significant compared to the control group (MD = -0.08; 95% CI: -0.27, 0.11; P = 0.01; I2 = 69.7%, Figure S6). NMA-based concordance analysis showed that aerobic activities (MD = -0.2, 95% CI: -0.47, 0.07), resistance activities (MD = -0.1, 95% CI: -0.45, 0.26), and standing (MD = 0.2, 95% CI: -0.26, 0.66) represented no statistically significant difference in results in comparison to the control group. Indirect comparisons demonstrated no statistically significant differences between the two sedentary interruption intercomparisons (Table S9). The effectiveness rank for improving carotid-to-radial PWV was standing (SUCRA = 0.844), resistance activities (SUCRA = 0.380), and aerobic activities (SUCRA = 0.144), respectively (Figure 3E).
Carotid-to-ankle PWV was reported in 5 studies involving 200 participants and four sedentary interruption interventions (i.e., aerobic activities, resistance activities, lower-extremity activities, and standing). Based on the results of the pairwise meta-analysis, sedentary interruption interventions effectively improved carotid-to-ankle PWV in the intervention group (MD = -1.12; 95% CI: -1.50, -0.73; P = 0.00; I2 = 97.2%, Figure S7). However, NMA-based concordance analysis showed that aerobic activities (MD = -0.14, 95% CI: -15.47, 15.21), lower-extremity activities (MD = 2.84, 95% CI: -8.01, 13.72), resistance activities (MD = -0.13, 95% CI: -15.42, 15.15) and standing (MD = -0.35, 95% CI: -15.67, 14.98) revealed no statistically significant difference in the results compared to the control group. Based on indirect comparisons, no statistically significant differences were observed between the two sedentary interruption intercomparisons (Table S9). The effectiveness rank for improving carotid-to-ankle PWV was lower-extremity activities (SUCRA = 0.656), resistance activities (SUCRA = 0.467), and aerobic activities (SUCRA = 0.465), respectively (Figure 3F).
Carotid-to-femoral PWV was found in 5 studies involving 190 participants and four sedentary interruption interventions (i.e., aerobic activities, resistance activities, lower-extremity activities, and standing). The results of the pairwise meta-analysis indicated that the sedentary interruption interventions were not statistically significant compared to the control group (MD = -0.01; 95% CI: -0.30, 0.28; P = 0.425; I2 = 0%, Figure S8). Based on NMA-based concordance analysis, aerobic activities (MD = -0.18, 95% CI: -15.46, 15.23), lower-extremity activities (MD = 2.83, 95% CI: -8.01, 13.69), resistance activities (MD = -0.11, 95% CI: -15.55, 15.21), and standing (MD = -0.31, 95% CI: -15.69, 15.04) demonstrated no statistically significant difference in results in comparison to the control group. Indirect comparisons showed no statistically significant differences between the two sedentary interruption intercomparisons. (Table S9). The effectiveness rank for improving carotid-to-femoral PWV was lower-extremity activities (SUCRA = 0.655), resistance activities (SUCRA = 0.467), and aerobic activities (SUCRA = 0.464), respectively (Figure 3G).
Publication Bias or Small Sample Effect Test
Funnel plots and Egger’s test were used to examine publication bias for indicators involved in this study (Figure 4A-D). Analyses for carotid-to-radial PWV, carotid-to-ankle PWV, and carotid-to-femoral PWV were not performed due to the limited number of studies. The funnel plots for all other indicators were basically symmetrical, and the Egger’s test utilized to assess publication bias suggested that P was more than 0.05 in all other indicators (Table S10), indicating that there was a low possibility of publication bias or a small sample effect in the current study.
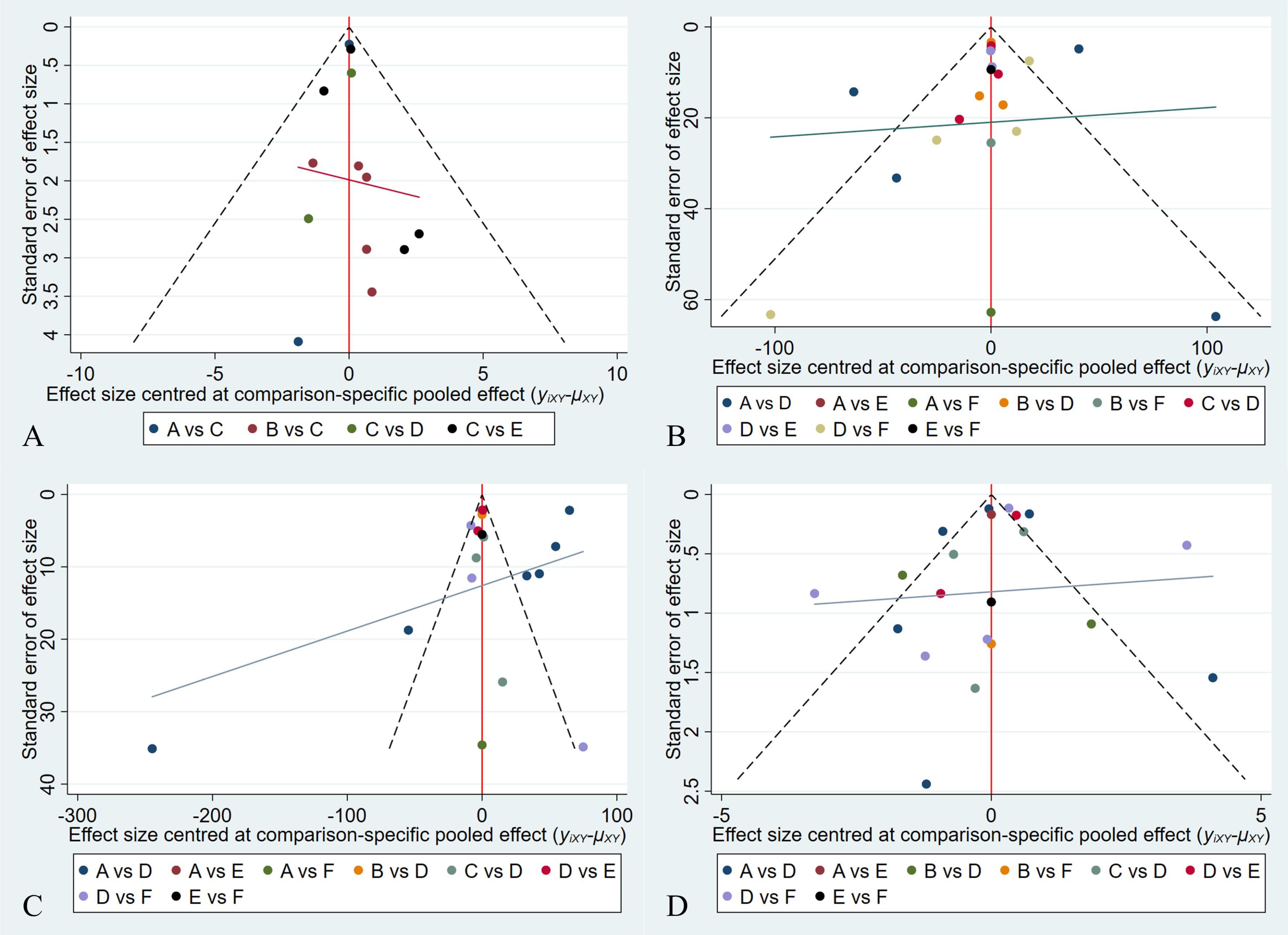
Figure 4.
Network Meta-Analysis Funnel Graph: Publication Bias or Small Sample Effect Test: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, and (D) Flow-Mediated Dilation%
.
Network Meta-Analysis Funnel Graph: Publication Bias or Small Sample Effect Test: (A) Mean Arterial Pressure, (B) Blood Flow, (C) Mean Arterial Shear Rate, and (D) Flow-Mediated Dilation%
Discussion
Currently, sedentary interruption has been established as an effective complementary therapy that can significantly improve arterial blood flow, shear rate, mean arterial pressure, and carotid-to-ankle PWV in sedentary populations (7,13). However, the effects of various types of sedentary interruption interventions on vascular health in adults exhibit inconsistencies. An NMA facilitates both direct and indirect comparisons of the effects of different sedentary interruption strategies, enabling the identification of the optimal approach.
Overall, sedentary interruption interventions can effectively improve the levels of blood flow, mean arterial shear rate, FMD%, and carotid-to-ankle PWV. Intermittent aerobic activity demonstrated significantly greater efficacy in improving blood flow, mean arterial shear rate, and mean arterial pressure compared to prolonged sitting and other interventions. Intermittent lower-extremity activities were found to be more effective than prolonged sitting and other sedentary interruption measures in improving FMD%. Additionally, aerobic activities were the most effective intervention in improving mean arterial pressure, blood flow, and mean arterial shear rate. Lower-extremity activities were most effective in improving FMD%, carotid-to-ankle PWV, and carotid-to-femoral PWV, and standing could improve carotid-to-radial PWV.
The decreases in mean arterial pressure, blood flow, and mean arterial shear rate are contributing factors to endothelial dysfunction. Previous studies confirmed that prolonged sedentary behavior leads to significant reductions in lower limb blood flow and shear stress, resulting in leg endothelial dysfunction (29-31). In a seated position, lower limb skeletal muscle activity is significantly diminished compared to standing or exercising, likely leading to reduced blood flow to the lower extremities (32). Additionally, the lack of muscle contractions hampers effective blood propulsion in the lower limbs, increasing the risk of blood pooling (9). Research further indicated that the average baseline shear rate demonstrates a marked decline during specific periods of continuous sitting for three hours, which correlates with low leg blood flow (33).
The SUCRA analysis in this study revealed that intermittent aerobic activities are the optimal intervention for improving blood flow, mean arterial shear rate, and mean arterial pressure. The findings suggest that utilizing aerobic activity as a sedentary interruption can yield beneficial effects on vascular function. Notably, some studies reported no significant differences in outcomes between the intervention and control groups (15,34), which may be attributed to variations in intervention intensity across different studies. The NMA provides robust evidence for the benefits of intermittent aerobic activity in optimizing vascular function. For instance, stair climbing as a sedentary interruption significantly improved peripheral blood flow (P = 0.004) (13). Furthermore, a study comparing prolonged sitting to aerobics showed that the shear rate in the brachial artery significantly increased after each aerobics session compared to sedentary conditions (15). These studies further underscore the critical importance and effectiveness of intermittent aerobic activity in maintaining vascular health.
FMD is a non-invasive indicator of cardiovascular health (endothelial function) and can effectively predict the occurrence of CVDs (35). Some studies have confirmed that sedentary interruption can significantly improve FMD (36,37). However, recent research by Taylor et al indicated a lack of a significant effect of intermittent breaks on FMD (SMD = 0.13) (8), highlighting discrepancies and controversies in prior findings regarding the impact of sedentary interruption on FMD. Moreover, a study comparing upper and lower limb flow-mediated vasodilation found that sedentary interruption interventions may be more effective in improving lower limb arterial dilation (1.60%) compared to upper limb arteries (1.19%) (17), suggesting that lower limb vascular health should be a priority focus. Our SUCRA analysis identified intermittent lower-extremity activities as the optimal intervention strategy for enhancing FMD%. This finding not only confirms the positive impact of sedentary interruption on endothelial function but also underscores the importance of targeted intervention strategies. Given the lack of specific treatments for endothelial dysfunction, this discovery offers an effective sedentary interruption approach for patients with endothelial dysfunction.
PWV serves as a non-invasive indicator of arterial stiffness and has been identified as an independent predictor of cardiovascular event risk. Research indicates that prolonged sedentary behavior, lasting up to three hours, can elevate PWV from the carotid to the femoral artery by approximately 0.3–0.4 m/s in healthy adults (38). This finding emphasizes the rapid adverse effects of sedentary behavior on vascular health. The findings of this study confirmed that sedentary breaks could improve the carotid-to-ankle PWV. However, current research on the impact of sedentary interruption interventions on PWV is still insufficient. Among the existing relevant studies, a study on the alternation between sitting and standing showed that intermittent standing could significantly improve the carotid-ankle PWV (7), which reflects the positive effect of this simple and easy sedentary interruption method on vascular health. In addition, another study compared active lower-extremity activities, passive lower-extremity activities, and the sedentary control group and reported that active lower-extremity activities could reduce the levels of carotid-to-ankle PWV and carotid-to-radial PWV, yet there was no significant difference among the groups (34). This implies that although active lower-extremity activities tend to improve PWV, they may not be sufficient to produce obvious differences among groups due to factors such as the intensity and duration of the intervention. It is worth mentioning that this result is also consistent with some of the conclusions drawn in this study, further confirming the complexity of the impact of different sedentary interruption methods on PWV. Some studies demonstrated that physical activity positively influences PWV, with a significant negative correlation between activity intensity and carotid-to-femoral PWV (39). Nonetheless, some sedentary interruption interventions have not effectively reduced PWV, which may suggest that the current sedentary interruption intervention methods might lack sufficient intensity and necessary duration, and thus have difficulty effectively counteracting the increase in PWV caused by prolonged sitting. Consequently, these interventions have limited effects on alleviating the harmful impacts brought about by arterial stiffness. Perhaps more vigorous and intensive physical activity interventions are required to counteract the increase in PWV. In conclusion, given that the current research on the impact of sedentary interruption on PWV is rather limited both in quantity and depth, it is necessary to conduct more in-depth and comprehensive studies in this regard in the future.
Limitations of the Study
This study had several limitations. Firstly, although the selected studies included RCTs and randomized crossover trials, the feasibility of blinding was compromised due to the nature of the research question, which may introduce potential bias into the findings. Secondly, the influence of critical factors, such as exercise intensity, frequency, and duration, on the outcomes was not sufficiently explored, potentially limiting the comprehensiveness of the results. Furthermore, while the core focus of this research was on the effects of sedentary interruption interventions on vascular health, other factors, such as disease status and dietary patterns, are closely related to determining the optimal approach for sedentary interruption interventions and should be evaluated in future studies. Lastly, the limited number of studies included on PWV constrained the ability to assess publication bias.
Conclusion
Sedentary interruption interventions may represent an effective and proactive strategy, particularly beneficial for sedentary populations, with the potential to significantly improve risk factors associated with CVDs and metabolic syndrome. Aerobic activities could be an ideal intervention for regulating mean arterial pressure, blood flow, and mean arterial shear rate. Additionally, lower-extremity activities demonstrate more pronounced benefits in enhancing FMD%. This study provides guidance for selecting appropriate sedentary interruption methods for sedentary individuals and offers a reference for further research.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
Not applicable. This study did not involve experiments on human or animal subjects and did not require the approval of the ethics committee.
Funding
The authors declare that they received no funding from any source.
Supplementary Files
Supplementary file 1 contains Tables S1-S10 and Figures S1-S8.
(pdf)
References
- Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act 2017; 14(1):75. doi: 10.1186/s12966-017-0525-8 [Crossref] [ Google Scholar]
- Rosenkranz SK, Mailey EL, Umansky E, Rosenkranz RR, Ablah E. Workplace sedentary behavior and productivity: a cross-sectional study. Int J Environ Res Public Health 2020; 17(18):6535. doi: 10.3390/ijerph17186535 [Crossref] [ Google Scholar]
- Whitaker KM, Pettee Gabriel K, Buman MP, Pereira MA, Jacobs DR Jr, Reis JP. Associations of accelerometer-measured sedentary time and physical activity with prospectively assessed cardiometabolic risk factors: the CARDIA study. J Am Heart Assoc 2019; 8(1):e010212. doi: 10.1161/jaha.118.010212 [Crossref] [ Google Scholar]
- Chen Y, Chan S, Bennett D, Chen X, Wu X, Ke Y. Device-measured movement behaviours in over 20,000 China Kadoorie Biobank participants. Int J Behav Nutr Phys Act 2023; 20(1):138. doi: 10.1186/s12966-023-01537-8 [Crossref] [ Google Scholar]
- Peter-Marske KM, Evenson KR, Moore CC, Cuthbertson CC, Howard AG, Shiroma EJ. Association of accelerometer-measured physical activity and sedentary behavior with incident cardiovascular disease, myocardial infarction, and ischemic stroke: the women’s health study. J Am Heart Assoc 2023; 12(7):e028180. doi: 10.1161/jaha.122.028180 [Crossref] [ Google Scholar]
- Bahls M, Leitzmann MF, Karch A, Teumer A, Dörr M, Felix SB. Physical activity, sedentary behavior and risk of coronary artery disease, myocardial infarction and ischemic stroke: a two-sample Mendelian randomization study. Clin Res Cardiol 2021; 110(10):1564-73. doi: 10.1007/s00392-021-01846-7 [Crossref] [ Google Scholar]
- Barone Gibbs B, Kowalsky RJ, Perdomo SJ, Taormina JM, Balzer JR, Jakicic JM. Effect of alternating standing and sitting on blood pressure and pulse wave velocity during a simulated workday in adults with overweight/obesity. J Hypertens 2017; 35(12):2411-8. doi: 10.1097/hjh.0000000000001463 [Crossref] [ Google Scholar]
- Taylor FC, Pinto AJ, Maniar N, Dunstan DW, Green DJ. The acute effects of prolonged uninterrupted sitting on vascular function: a systematic review and meta-analysis. Med Sci Sports Exerc 2022; 54(1):67-76. doi: 10.1249/mss.0000000000002763 [Crossref] [ Google Scholar]
- Morishima T, Restaino RM, Walsh LK, Kanaley JA, Fadel PJ, Padilla J. Prolonged sitting-induced leg endothelial dysfunction is prevented by fidgeting. Am J Physiol Heart Circ Physiol 2016; 311(1):H177-82. doi: 10.1152/ajpheart.00297.2016 [Crossref] [ Google Scholar]
- Jenkins NT, Padilla J, Boyle LJ, Credeur DP, Laughlin MH, Fadel PJ. Disturbed blood flow acutely induces activation and apoptosis of the human vascular endothelium. Hypertension 2013; 61(3):615-21. doi: 10.1161/hypertensionaha.111.00561 [Crossref] [ Google Scholar]
- Dempsey PC, Biddle SJ, Buman MP, Chastin S, Ekelund U, Friedenreich CM. New global guidelines on sedentary behaviour and health for adults: broadening the behavioural targets. Int J Behav Nutr Phys Act 2020; 17(1):151. doi: 10.1186/s12966-020-01044-0 [Crossref] [ Google Scholar]
- Garcia JM, Duran AT, Schwartz JE, Booth JN 3rd, Hooker SP, Willey JZ. Types of sedentary behavior and risk of cardiovascular events and mortality in Blacks: the Jackson Heart Study. J Am Heart Assoc 2019; 8(13):e010406. doi: 10.1161/jaha.118.010406 [Crossref] [ Google Scholar]
- Cho MJ, Bunsawat K, Kim HJ, Yoon ES, Jae SY. The acute effects of interrupting prolonged sitting with stair climbing on vascular and metabolic function after a high-fat meal. Eur J Appl Physiol 2020; 120(4):829-39. doi: 10.1007/s00421-020-04321-9 [Crossref] [ Google Scholar]
- Kruse NT, Hughes WE, Benzo RM, Carr LJ, Casey DP. Workplace strategies to prevent sitting-induced endothelial dysfunction. Med Sci Sports Exerc 2018; 50(4):801-8. doi: 10.1249/mss.0000000000001484 [Crossref] [ Google Scholar]
- Carter SE, Gladwell VF. Effect of breaking up sedentary time with callisthenics on endothelial function. J Sports Sci 2017; 35(15):1508-14. doi: 10.1080/02640414.2016.1223331 [Crossref] [ Google Scholar]
- Carter SE, Draijer R, Holder SM, Brown L, Thijssen DH, Hopkins ND. Effect of different walking break strategies on superficial femoral artery endothelial function. Physiol Rep 2019; 7(16):e14190. doi: 10.14814/phy2.14190 [Crossref] [ Google Scholar]
- Zheng C, Zhang X, Sheridan S, Ho RS, Sit CH, Huang Y. Effect of sedentary behavior interventions on vascular function in adults: a systematic review and meta-analysis. Scand J Med Sci Sports 2021; 31(7):1395-410. doi: 10.1111/sms.13947 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71 [Crossref] [ Google Scholar]
- Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 2015; 162(11):777-84. doi: 10.7326/m14-2385 [Crossref] [ Google Scholar]
- Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366:l4898. doi: 10.1136/bmj.l4898 [Crossref] [ Google Scholar]
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014; 14:135. doi: 10.1186/1471-2288-14-135 [Crossref] [ Google Scholar]
- Higgins JP, Li T, Deeks JJ. Choosing effect measures and computing estimates of effect. In: Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019. p. 143-76. doi: 10.1002/9781119536604.ch6.
- Bois FY. Bayesian inference. Methods Mol Biol 2013; 930:597-636. doi: 10.1007/978-1-62703-059-5_25 [Crossref] [ Google Scholar]
- Hamra G, MacLehose R, Richardson D. Markov chain Monte Carlo: an introduction for epidemiologists. Int J Epidemiol 2013; 42(2):627-34. doi: 10.1093/ije/dyt043 [Crossref] [ Google Scholar]
- Dias S, Sutton AJ, Welton NJ, Ades AE. Heterogeneity: Subgroups, Meta-Regression, Bias and Bias-Adjustment [Internet]. London: National Institute for Health and Care Excellence (NICE); 2012.
- Veroniki AA, Vasiliadis HS, Higgins JP, Salanti G. Evaluation of inconsistency in networks of interventions. Int J Epidemiol 2013; 42(1):332-45. doi: 10.1093/ije/dys222 [Crossref] [ Google Scholar]
- Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol 2011; 64(2):163-71. doi: 10.1016/j.jclinepi.2010.03.016 [Crossref] [ Google Scholar]
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315(7109):629-34. doi: 10.1136/bmj.315.7109.629 [Crossref] [ Google Scholar]
- Restaino RM, Walsh LK, Morishima T, Vranish JR, Martinez-Lemus LA, Fadel PJ. Endothelial dysfunction following prolonged sitting is mediated by a reduction in shear stress. Am J Physiol Heart Circ Physiol 2016; 310(5):H648-53. doi: 10.1152/ajpheart.00943.2015 [Crossref] [ Google Scholar]
- McManus AM, Ainslie PN, Green DJ, Simair RG, Smith K, Lewis N. Impact of prolonged sitting on vascular function in young girls. Exp Physiol 2015; 100(11):1379-87. doi: 10.1113/ep085355 [Crossref] [ Google Scholar]
- Thosar SS, Bielko SL, Mather KJ, Johnston JD, Wallace JP. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med Sci Sports Exerc 2015; 47(4):843-9. doi: 10.1249/mss.0000000000000479 [Crossref] [ Google Scholar]
- Restaino RM, Holwerda SW, Credeur DP, Fadel PJ, Padilla J. Impact of prolonged sitting on lower and upper limb micro- and macrovascular dilator function. Exp Physiol 2015; 100(7):829-38. doi: 10.1113/ep085238 [Crossref] [ Google Scholar]
- Shvartz E, Gaume JG, White RT, Reibold RC. Hemodynamic responses during prolonged sitting. J Appl Physiol Respir Environ Exerc Physiol 1983; 54(6):1673-80. doi: 10.1152/jappl.1983.54.6.1673 [Crossref] [ Google Scholar]
- Park SY, Wooden TK, Pekas EJ, Anderson CP, Yadav SK, Slivka DR. Effects of passive and active leg movements to interrupt sitting in mild hypercapnia on cardiovascular function in healthy adults. J Appl Physiol (1985) 2022; 132(3):874-87. doi: 10.1152/japplphysiol.00799.2021 [Crossref] [ Google Scholar]
- Calderón-Gerstein WS, López-Peña A, Macha-Ramírez R, Bruno-Huamán A, Espejo-Ramos R, Vílchez-Bravo S. Endothelial dysfunction assessment by flow-mediated dilation in a high-altitude population. Vasc Health Risk Manag 2017; 13:421-6. doi: 10.2147/vhrm.S151886 [Crossref] [ Google Scholar]
- Paterson C, Fryer S, Zieff G, Stone K, Credeur DP, Barone Gibbs B. The effects of acute exposure to prolonged sitting, with and without interruption, on vascular function among adults: a meta-analysis. Sports Med 2020; 50(11):1929-42. doi: 10.1007/s40279-020-01325-5 [Crossref] [ Google Scholar]
- Soto-Rodríguez FJ, Cabañas EI, Pérez-Mármol JM. Impact of prolonged sitting interruption strategies on shear rate, flow-mediated dilation and blood flow in adults: a systematic review and meta-analysis of randomized cross-over trials. J Sports Sci 2022; 40(14):1558-67. doi: 10.1080/02640414.2022.2091347 [Crossref] [ Google Scholar]
- Credeur DP, Miller SM, Jones R, Stoner L, Dolbow DR, Fryer SM. Impact of prolonged sitting on peripheral and central vascular health. Am J Cardiol 2019; 123(2):260-6. doi: 10.1016/j.amjcard.2018.10.014 [Crossref] [ Google Scholar]
- Germano-Soares AH, Andrade-Lima A, Menêses AL, Correia MA, Parmenter BJ, Tassitano RM. Association of time spent in physical activities and sedentary behaviors with carotid-femoral pulse wave velocity: a systematic review and meta-analysis. Atherosclerosis 2018; 269:211-8. doi: 10.1016/j.atherosclerosis.2018.01.009 [Crossref] [ Google Scholar]